This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia.
This post will focus on the key parts of the guideline that affect ED evaluation and management. Vasopressor medications during cardiac arrest We recommend that epinephrine be administered for patients in cardiac arrest. It is reasonable to administer epinephrine 1 mg every 3 to 5 minutes for cardiac arrest. COR 1, LOE B-R.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S. Circulation.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). This patient is actively dying from a left main coronary artery OMI and cardiac arrest from VT/VF or PEA is imminent!
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade Ann Int Med 897-903 112 12 1990 December 15 816 2 style='mso-element:field-end'> Indeed, major articles advising against the use of beta blockers in cocaine toxicity reference only this article and do not discuss cardioselectivity. Cigarroa, R.G. McBride, W.
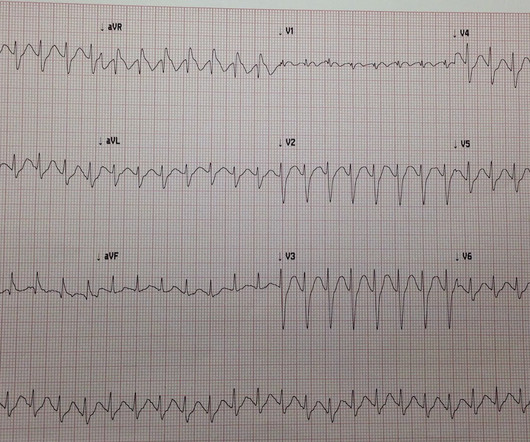
With ventilations and epinephrine, she regained a pulse. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. BP gradually rose.
Fine ventricular fibrillation She received 2 mg epinephrine, 150 mg amiodarone and underwent chest compressions with the LUCAS device. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Updates on the Electrocardiogram in Acute Coronary Syndromes. The patient was discharged neurologically intact.
She was given 3 mg IV epinephrine and multiple rounds of ACLS over approximately 20 minutes. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). She was never defibrillated.
They stated that the patient was coded for 20 minutes, including multiple doses of epinephrine, and they also gave glucose, calcium, and bicarb. As stated above, resuscitation included epinephrine, calcium, and bicarb. Acute coronary syndrome is unlikely to be one of those entities. After ROSC achieved: Sinus rhythm.
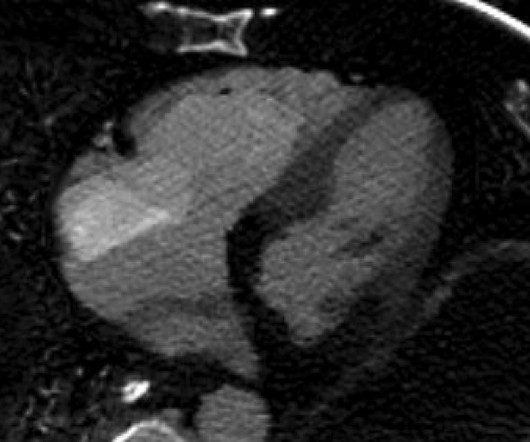
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. In the cath lab, the patient’s blood pressure remained low.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. And so it is wise to look at the coronary arteries. He was moderately hypoxic.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. On epinephrine and norepinephrine drips." CPR was initiated immediately. CT angiogram showed extensive saddle pulmonary embolism.
Here is his ED ECG: There is obvious infero-posterior STEMI. Over a 13-month period, serum potassium and magnesium levels were measured in 590 patients admitted to a coronary care unit. Medics stated that he had not been taking his clopidogrel for 2 weeks. He appeared to be in shock. What are you worried about in addition to his STEMI?
The catheterization lab is activated, but catheterization shows no coronary artery occlusion. ECG shows ST-segment elevation in V3-V6 only with depression in aVR. Initial troponin is mildly elevated. On further questioning, the patient denies recent illness but does mention that her daughter passed away in a car accident yesterday.
Sex ed” sucks. They believe that Sex Ed programs are irrelevant to real-life experience and contain inadequate discussion of important issues, including consent or positive sexual relationships. Both were partly delivered via caesarian section, flow probes inserted into carotid, pulmonary and left circumflex coronary arteries.
We talk about the nitty-gritty details of a well-run cardiac arrest, with Scott Weingart of Emcrit (@emcrit), ED intensivist. Takeaway lessons Resources We talk about the nitty-gritty details of a well-run cardiac arrest, with Scott Weingart of Emcrit ( @emcrit ), ED intensivist. Learn more at the Intensive Care Academy!
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. Resuscitated with chest compressions, epinephrine. including epinephrine, and there was ROSC. Moreover, it does not follow a coronary distribution very well.
On arrival to the ED, he was breathing spontaneously, had faint pulses, and was cool to the touch. He was given 50 mcg epinephrine with good response in both heart rate and blood pressure. His heart rate had improved to the 80s after epinephrine administration. Epinephrine drip was started and norepinephrine was discontinued.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. EPINEPHRINE-INUDCED SHOCK: LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION ON VASOPRESSORS. Clin Cardiol. 2009;32(7):397-402.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content