This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. The ED activated trauma services, and a 12 Lead ECG was captured. The fall was not a mechanical etiology.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
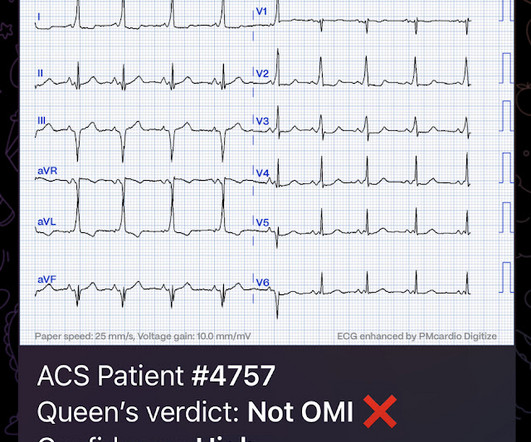
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
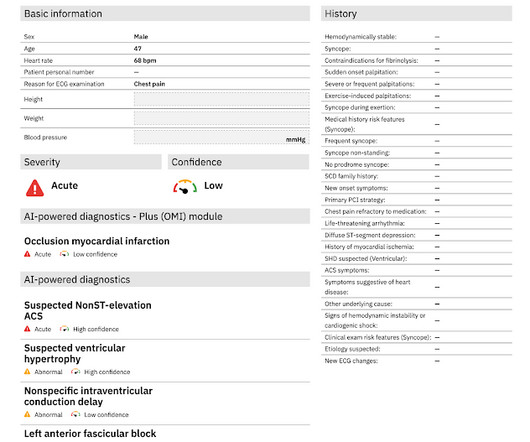
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
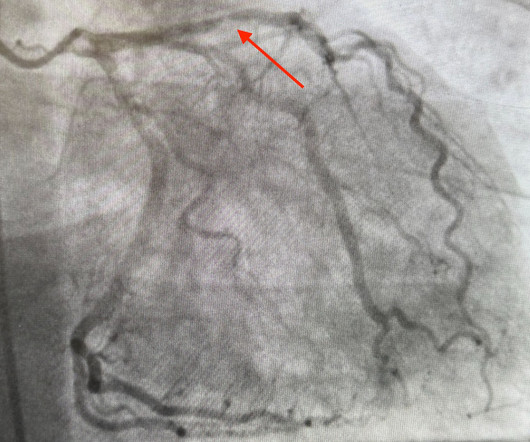
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification. Cardiol Rev.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chest pain around 1500 while eating. Patient 2 , EKG 1: What do you think? He went to the cath lab at 0900 the next morning.
He called EMS who brought him to the ED. ED Diagnoses: 1. The basic principles of emergency ECG interpretation in patients who present to an ED with new symptoms include the following: Respect the History. This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents.
JAMA Intern Med 2021 Case: A 60-year-old man presents to the emergency department (ED) after his wife found him to be drowsy and confused at home. On arrival to the ED his vitals are normal aside from a decreased level of consciousness and he is found to have a serum sodium concentration of 118 mmol/L.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
It was present on arrival at triage but then resolved before bed placement in the ED. This is a demonstration of how Wellens' is transient OMI : First ED ECG is Wellens' (pain free). Also see this incredible case of the use of 12-lead ST Segment monitoring. __ Case Continued The Cath lab was activated 70 minutes after ED arrival.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. Here is his ED ECG: What do you think? Smith offers the unique perspective of assessing the initial ECG of a patient who has had prior events — and, who now presents with new symptoms.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. No ECG was ordered on Day #1.
Coronaries were clean. ECG Features suggesting "Fake" As per Dr. Sam Ghali ( who sent us today's case ) — serial Troponins were clearly indicated since the patient presented to the ED. Negative serial Troponins were needed to rule out an acute event. Sam : "Yes, this case was sent to me. It was a man in his 30s with chest pain.
Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. This study failed to do so.
When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. But I'd be less certain about an acute event without more information and prior and/or serial tracings. It is unknown when this pain recurred and became constant.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
Beats 9-12 : Continuation of the previously described events, all inducible by the pause (and thus, prolongation of refractoriness) created by the PVC of Beat 8. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Chou’s Electrocardiography in Clinical Practice (6th ed). Surawicz, B.
Here is his initial ED ECG: What do you think? Then the ED doc would be dependent on that first ECG. It must have re-occluded between the ED and the cath lab) --Lesion was stented. have perfect coronary flow by the time of angiogram. Or had not had a prehospital ECG on the ambulance.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. For the same reason, you should not delay coronary angiography because pain resolves with morphine. But pain is a critical signal for urgency in the context of acute coronary syndrome. Mukherjee, D.,
This particular facility is situated for independent living, thus no medical providers are on site to provide pertinent details for medical history, medication intake, or remarkable events prior to the incident at hand. Josephson’s Clinical Cardiac Electrophysiology: Techniques and Interpretations (6th ed). 2] Viskin, S., 8] Liu, E.,
There was no association between moderate to severe chest pain on arrival and major adverse cardiac events at 6 months (20% vs. 14%, p=0.12). Having severe pain drives people to the ED for faster treatment! Chest pain severity was assessed upon admission to the primary percutaneous coronary intervention hospital. years old ± 13.7
He reported typical chest pain since 4H AM and arrived at our ED at 10h with ongoing chest pain. The coronary angiography showed a 100% ostial main (obtuse) marginal occlusion!" Dominant right coronary, atherosclerotic and calcified. Presence of a single coronary lesion: occlusion of the ostial main marginal.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? See these casese (and I have many others): First ED ECG is Wellens' (pain free). A 70-something y.o. male presents to triage with shortness of breath.
link] A 30 year-old woman was brought to the ED with chest pain. The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This is written by Brooks Walsh.
Imagine you just started your ED shift. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. R wave V4 9mm) C T of the coronary arteries showed no lesions. That said, this patient did present to the ED with "new CP" — and.
I interpreted this tracing knowing only that the patient was a woman in her 60s, with a prior history of proximal LAD OMI — who now presented to the ED with a history of new chest discomfort and shortness of breath. For clarity in Figure-1 — I’ve labeled today’s initial tracing. Figure-1: I've labeled the initial ECG in today's case.
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). 3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013.
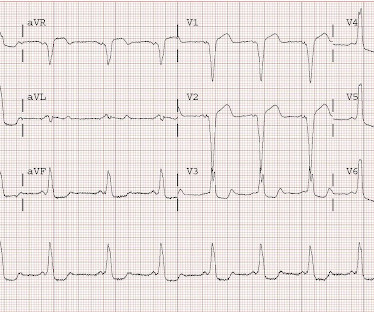
He subsequently had a syncopal event and was down for 1-2 minutes. Upon arrival to the ED, he had the following 12-lead ECG: There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF. His wife called 911. EMS found him with an irregular heart rate at 200-250 beats per minute.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings. Attached is the first ECG. 3] Smith, S.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. In the ED, ultrasound showed hemopericardium with tamponade.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. Finally, coronary angiography was performed (at least 5 days after presentation) which confirmed LAD aneurysm with large thrombus burden, TIMI 0 flow, thrombectomy performed.
About an hour later, he was then found on the floor in cardiac arrest in the ED. The history in today's case — was that of a man in his 70s who presented to the ED for 2 hours of chest pain , that was still present on arrival in the ED. His initial troponin T was 15 ng/L (only two hours since pain onset).
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. Prevalence of Total Coronary Occlusion during the Early Hours of Transmural Myocardial Infarction. Computerized QTc = 419.
Takotsubo is a sudden event, not one with crescendo angina. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 Next day, t he patient was taken for an angiogram and found to have a reperfused LAD lesion with good flow that appeared to the angiographer as if it was a spontaneous coronary artery dissection. She felt more comfortable being admitted.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. Apparently, the patient was not satisfied, and came to the ED as he still had pain. It was extremely busy in the ED and things did not get done quickly. This middle-aged male with known coronary disease presented with new chest pain.
Emergent CT coronary angio also likely has a role in such cases. Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content