This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
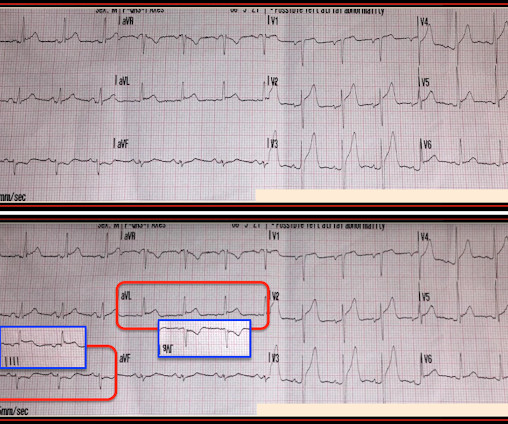
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
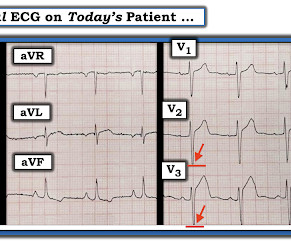
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. The young ED tech immediately suspected LAD OMI.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (Ret) @DidlakeDW Expert contribution by Dr Robert Herman @RobertHermanMD @PowerfulMedical (Chief Medical Officer) An adult male called 911 for new-onset epigastric burning. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
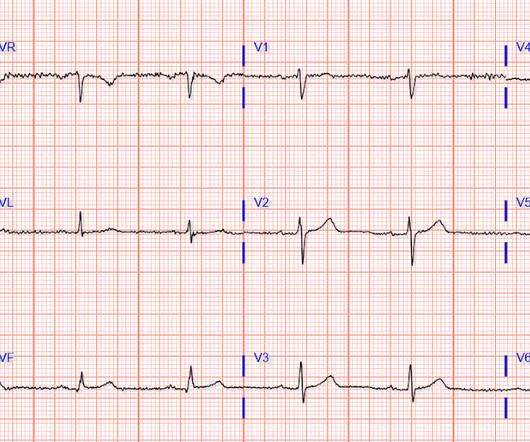
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. Below is the initial ED ECG. It is spread to V2 and V3.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. In isolation this ECG does not show OMI, but following the paramedic ECGs this indicates spontaneous LAD reperfusion. It’s unclear if the paramedic ECGs were seen or missed in the ED.
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease. Pharmacology Review Digoxin is probably one of those medications vaguely recalled from paramedic school.
Madden, Paramedic. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). An interesting comment provided by Paramedic Madden is that a few team members initially interpreted the T wave presentation as hyperkalemia, as opposed to occlusive hyperacuity. Physiology.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. Pertinent medical history includes HTN, HLD, and DM – all of which are optimally controlled with medication.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic @DidlakeDW A 50 y/o Male was taking his dog for a leisurely stroll through the park when he suddenly experienced new onset chest discomfort. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. Here is the final ECG just prior to ED transfer. It’s important to stress the presence of a normal QRS (i.e.,
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGBlog An adult female called 911 for chest discomfort and difficulty breathing. The following ECG was captured upon arrival at the receiving ED. The ED resulted an 8.7 The serum K returned 8.7,
But the paramedic and the ED physician in this case did not subscribe to this idea. It is far too premature to say that paramedics and physicians should not be bothered to interpret ECGs labelled as "normal" or "otherwise normal" by the computer algorithm. Thus, this is obvious STEMI(+) OMI until proven otherwise.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. 1] Here is the admitting ED ECG after cancellation of Code STEMI. 1] Driver, B.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Chou’s Electrocardiography in Clinical Practice (6th ed). Surawicz, B. & Knilans, T.
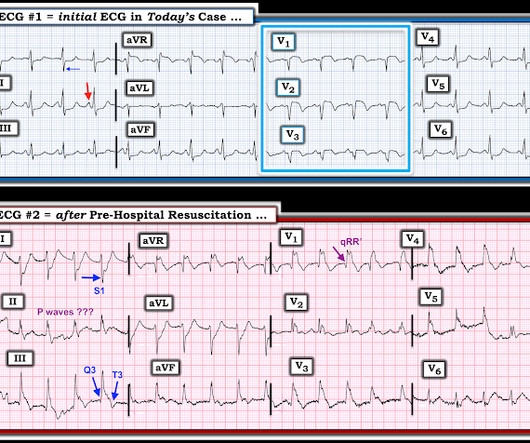
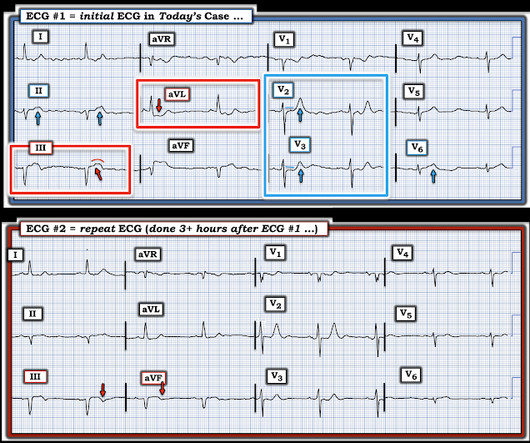
An ED ECG, if recorded with pain, should show LAD OMI. Smith — in the setting of a patient with new chest pain — the initial ECG in today's case ( = ECG #1 — obtained by the EMS team prior to ED arrival ) — is diagnostic of ACS ( A cute C oronary S yndrome ) until proven otherwise.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Coronaries were normal, as was serial troponin. Vitals were normal.
[link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. On arrival in the ED, the patient denied any symptoms at all. No chest pain, no shortness of breath, no back pain, no numbness, weakness, tingling, no seizures or history of seizures, First ED ECG This still shows apparent inferior OMI.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. Chou’s Electrocardiography in Clinical Practice, 6th ed. Goldberger’s Clinical Electrocardiography: A Simplified Approach, 9th ed.
They arrived in the ED 30 minutes later to meet the cardiology team, where an ECG was repeated: Again no STEMI criteria, and there has been improvement in the deWinter and swirl pattern. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
She went to angio and had normal coronaries. Paramedics found her semi-conscious, pale, cool, diaphoretic, tachypneic, very hypotensive. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries. I discussed the case with Cardiology will admit to their service."
This was shown to me by a very astute Hennepin paramedic. Although this comes from a Hennepin paramedic, the patient was not brought to Hennepin County Medical Center. It is important for cardiologists to realize that a paramedic may see something they do not. For some reason unknown to me, the interventionalist was in the ED.
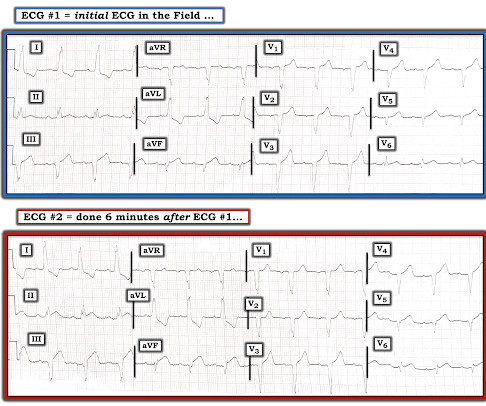
Written by Jesse McLaren Two 70 year olds had acute chest pain with nausea and shortness of breath, and called paramedics. But these ECGs were from the same patient: #1 on paramedic arrival and #2 thirty minutes later. Thankfully this patient’s second ECG met STEMI criteria, so paramedics brought them as a code STEMI.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. One need not have obstructive coronary disease to have occlusive thrombus!
The paramedic recorded a series of ECGs; the initial ECG is representative here: Computer read: “ Normal ECG ” What do you think? He was almost asymptomatic when he arrived in the ED. The paramedic interpreted this as a STEMI. An ECG was obtained in the ED: There is ST elevation in V2-V4. The ED ECG is more equivocal.
The symptoms improved somewhat after the paramedic gave her nitroglycerin. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? Despite the computer interpretation, the ED physician was concerned about the ECG, and planned for serial troponins.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. 2 The astute paramedic recognized this possibility and announced a CODE STEMI.
This case was sent by Lou B, a paramedic and RN. The coronaries were clean (this is not the gold standard, however, as some patients with ischemic ST elevation may have clean coronaries). ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery.
The paramedics found the patient with ROSC and a GCS 7, and an ECG showing LBBB with possible lateral ST elevation. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Below is the first ED ECG, labeled LBBB by the machine. Vitals were HR 58 BP 167/70 R20 sat 96%.
Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them.
Her initial 12-lead ECG that was obtained by paramedics in the field is shown in Figure-1. Figure-1: The initial ECG in todays case, obtained by paramedics in the field. ( NOTE: Because LBBB changes the sequence of LV repolarization it may be more difficult to recognize acute coronary occlusion on ECG. See text ). ( See text ).
Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them.
When the paramedics arrived, they obtained a 12 lead ECG and confirmed the unstable vital signs. Also, the RV appears large and hypokinetic The patient kept having recurrent syncopal episodes in the ED and was subsequently intubated for stabilization and airway protecting prior to going to the cath lab. Why is the patient in shock?
Here’s the paramedic ECG (digitized by PMcardio). According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. HR 40, BP 135/70, RR16, O2 100%. What do you think?
This was texted to me by a paramedic while I was out running one day: "54 yo male chest pain started at 1pm. I found out that the interventionalist had just finished a case and came to the ED to see about the de-activated case. He saw the ECG and ordered an ED ECG." History of diabetes type II and stent placement in 2018.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. The coronaries were clean. From this site.
She was found by paramedics with an oxygen saturation of 64%, but could not tolerate BiPAP during transport due to claustrophobia. She arrived to the ED with a nonrebreather mask. The ED physician noted Once her respiratory status improved, her EKG looks much improved with no evidence of STEMI. An EKG was immediately recorded.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. He presented to a rural ED at approximately 0630hrs.
Pretty impressive for someone who has not yet attended med school, or even been a nurse or paramedic yet. He was worked up non-emergently in the ED with pain recurring and resolving multiple times during his stay. En route to the next hospital, the paramedics recorded another 12-lead tracing. Another EKG was eventually taken.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chest pain that started while working at his desk. The paramedic thought it was LAD OMI, but wasn't certain. The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content