This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. We looked at 101 STEMI patients from two rural EDs. Date: November 22, 2023 Reference: Stopyra et al.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Post Created By: William Caputo MD Post Peer Reviewed By: Anand Swaminathan MD, MPH (Twitter @EMSwami ) The post REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion appeared first on REBEL EM - Emergency Medicine Blog.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
The Case A 62-year-old male with a history of Hypertension, Hyperlipidemia, Coronary Artery Disease with stents, Pulmonary Embolism on Eliquis, presents with sudden onset, severe, mid-sternal chest pain that started 15 minutes prior to arrival. Serial ECG's should be obtained to assess for evolution to acute STEMI.
But do they represent acute coronary occlusion? But coronaries were normal, and serial high sensitivity troponin was undetectable. Based on ECG changes and echo findings, the patient was diagnosed as coronary vasospasm. Formal echo showed EF 55% with mild inferolateral hypokinesis without any prior for comparison.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. Fortunately the patient did not reocclude while awaiting the angiogram.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Breath sounds were clear in all lung fields.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." But troponin is a rear-view mirror which shows damage that has already occurred, and is often within the normal range within only 2 hours of onset of acute coronary occlusion.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. The young ED tech immediately suspected LAD OMI.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
It was present on arrival at triage but then resolved before bed placement in the ED. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). It is a ssociated with mild dyspnea on exertion. Aspirin given.
The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Cardiac arrest #3: ST depression, Is it STEMI? It also does not uniformly indicate severe coronary disease. sodium bicarbonate.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Having severe pain drives people to the ED for faster treatment! We analyzed 1409 STEMI activations (69% male, 66.3 years old ± 13.7
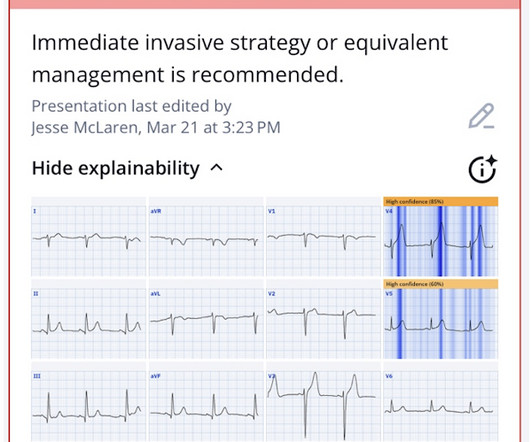
He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. ED Diagnoses: 1.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Here is the final ECG just prior to ED transfer. The pathology is now painfully evident.
1: How to Treat Infected Kidney Stones Spoon Feed All patients with infected ureteral stones necessitate a urine culture, antibiotics, and urology consultation in the ED, with the majority requiring admission for surgical intervention. Clay Smith at @spoonfedEM , and sign up for email updates here. #1:
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Smith Comment: Is is common for the artery to be open at angiogram in OMI, including full STEMI.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Here is his initial ED ECG: What do you think? Here it is: Obvious Inferior Posterior STEMI (+) OMI. Then the ED doc would be dependent on that first ECG. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. have perfect coronary flow by the time of angiogram.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. When EMS found her, she was dyspneic and diaphoretic.
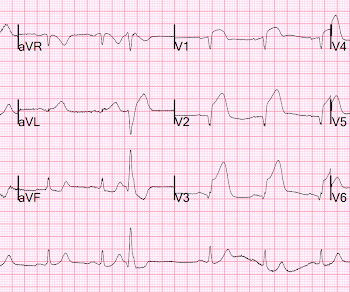
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." What do you think?
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." It is clearly missed by the conventional algorithm.
This post will focus on the key parts of the guideline that affect ED evaluation and management. Percutaneous coronary intervention after cardiac arrest Coronary angiography should be performed emergently for all cardiac arrest patients with suspected cardiac cause of arrest and ST-segment elevation on electrocardiogram.
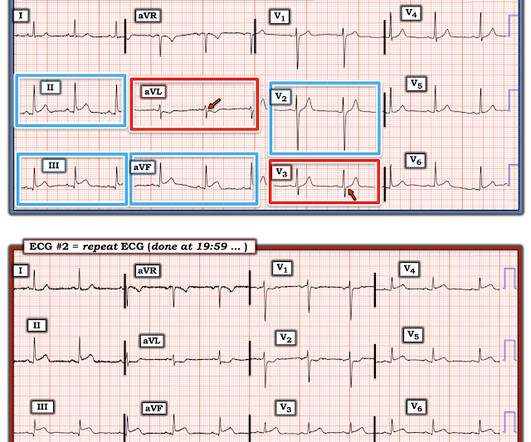
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." Transient STEMI is at high risk of re-occlusion.
Written by Bobby Nicholson What do you think of this “STEMI”? EKG on arrival to the ED is shown below: What do you think? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). or basilar ischemia.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. The patient was transported to the ED. Here is his ED ECG: There is sinus tachycardia. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
Jason was very skeptical of STEMI. Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. This also argues against STEMI. He complained of 3 days of diarrhea and abdominal pain.
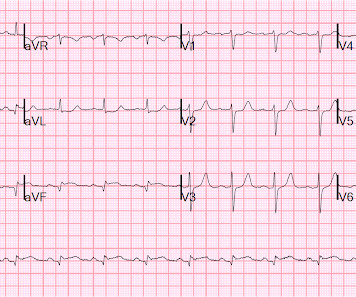
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. Leads II, III, aVF show about 0.5
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content