This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
On a busy day shift in the emergencydepartment, our seasoned triage nurse comes to me after I finish caring for a hallway patient, “Hey, can you come see this guy in the triage room? This is the essence of emergency medicine. The post Putting Clinical Gestalt to Work in the EmergencyDepartment appeared first on ACEP Now.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia.
Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk EmergencyDepartment Patients: The PROPER Randomized Clinical Trial. Case: A 47-year-old woman presents to the emergencydepartment with a 24-hour history of chest pain and shortness of breath. JAMA February 2018.
Date: June 14th, 2017 I had the pleasure of presenting at the Intra America Emergency Medicine Conference (#IAEMC17) held in Costa Rica last month. Thank you to Dr. Manrique Umana for inviting me and the conference organizers for putting on such an amazing and educational event.
He is a GP by training but works in EmergencyDepartment, Anaesthesia, Internal Medicine and Paediatrics. He has a wonderful #FOAMed blog and podcast called Broomedocs and also work […] The post SGEM#326: The SALSA Study: Hypertonic Saline to Treat Hyponatremia first appeared on The Skeptics Guide to Emergency Medicine.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). They too have dense white masses consistent with coronary atherosclerosis. The blue circle shows the LCx. Murakami MM.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Takotsubo is a sudden event, not one with crescendo angina. Such cases are classified as MINOCA (Myocardial Infarction with Non-Obstructed Coronary Arteries). It can only be seen by IVUS.
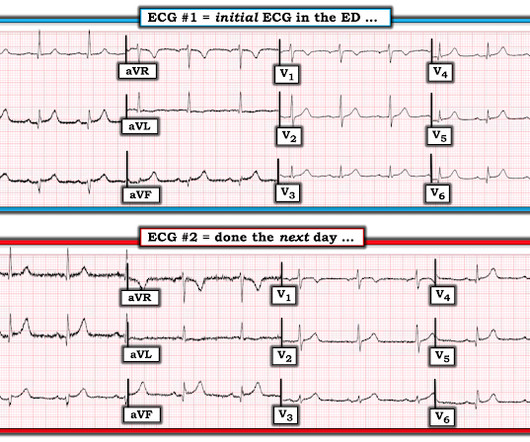
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. The undergraduate is now willing to identify himself: Hans Helseth. No ECG was ordered on Day #1.
ST segment elevation, or even an isoelectric ST segment, in these leads is abnormal and should make us concerned for ischemia Source Acute Coronary Occlusion in a Patient With Prior Known Right Bundle Branch Block: Another Chink in the Armor for the ST-Elevation Myocardial Infarction Criteria. Ann Emerg Med. 2023 Aug;82(2):219-221.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Background and Context Contrast-enhanced computed tomography (CECT) is of paramount importance in the emergencydepartment (ED) due to its indispensable role in facilitating precise diagnostic outcomes. Increased Computed Tomography Utilization in the EmergencyDepartment and Its Association with Hospital Admission.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
A prospective validation of the HEART score for chest pain patients at the emergencydepartment. External validation of the emergencydepartment assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP). Am J Emerg Med 2020 3. Backus BE, Six AJ, Kelder JC, et al. Int J Cardiol 2013 2. Lancet 2015 6.
It was ongoing on arrival in the emergencydepartment. STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. Am J Emerg Med 2023 2. What do you think?
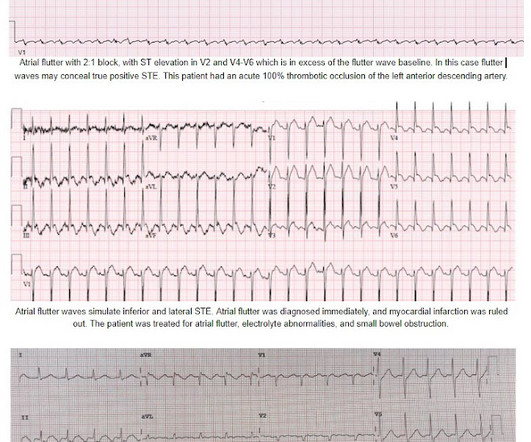
On arrival to the PCI center's EmergencyDepartment, the receiving team recorded an ECG on arrival: Persistent atrial flutter, however this time the QRS occurs on a slightly different portion of the flutter wave. No obvious adverse events were attributed to the thrombolytics. There was again no intracranial hemorrhage.
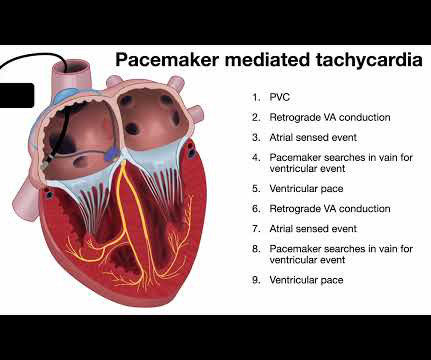
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The most recent event had occurred just before being triaged. Triage EKG: What do you think?
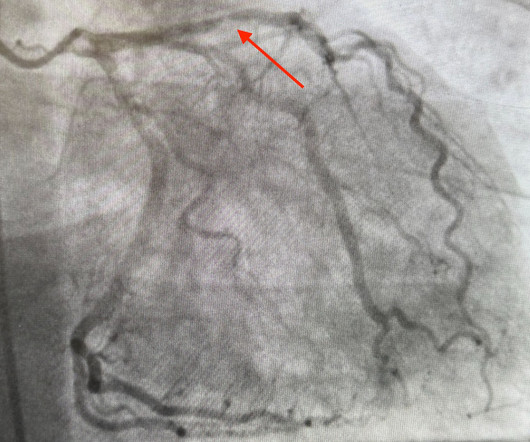
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Relationship between an in-farct related artery, acute total coronary occlusion, and mortality in patients with ST-segment and non-ST-segment myocardial infarction.
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
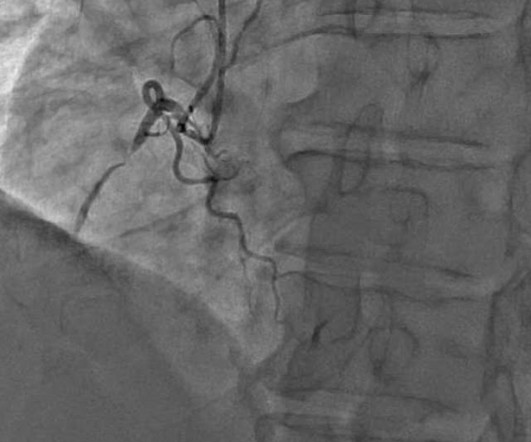
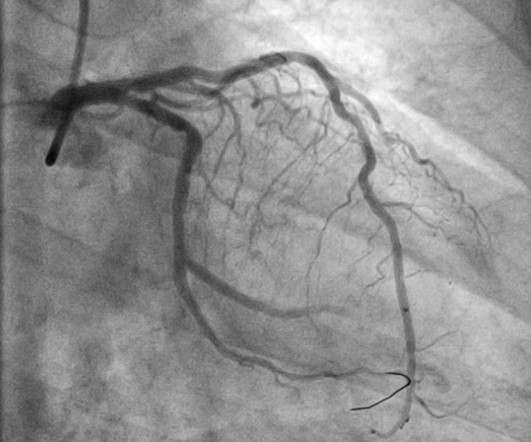
The patient’s ECG on arrival at the emergencydepartment is shown below. He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. In the available view, the RCA appears fully occluded.
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? The patient went emergently to the cath lab, where all coronary arteries were found to be normal.
The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. CASE #2: I am more disturbed by learning of the events associated with the ECG in Case #2.
This particular facility is situated for independent living, thus no medical providers are on site to provide pertinent details for medical history, medication intake, or remarkable events prior to the incident at hand. Unfortunately, a post-conversion 12 Lead was not acquired. This finding might favor a diagnosis of ischemic-driven PVT.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. STEMI criteria, and automated interpretations based on it, will miss acute coronary occlusion. Take home 1.
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Instead — it commonly reflects ischemia from severe underlying coronary disease. He did not have chest pain.
And so it is wise to look at the coronary arteries. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
But the bradycardia and the infero-posterior OMI is definitely new: Smith : this also has many abnormalities suggestive of ischemia: many leads have ischemic appearing ST depression The emergency provider followed the sequential steps of the current paradigm: 1.
If there is no defined injury or event that could have led to a soft tissue injury, we should be reluctant to render a diagnosis of musculoskeletal pain. Presenting complaint among patients with myocardial infarction who present to an urban, public hospital emergencydepartment. Ann Emerg Med 2002; 40:180–6.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e I B Patients transferred to PCI centres can bypass the emergencydepartment to undergo primary PCI without delay. STEMI , ST-segment elevation acute myocardial infarction ).
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Interventions during the acute phase of treatment post return of spontaneous circulation (ROSC) are therefore critical.
However, none of the formulas have proven to be definitively better than another and none are well correlated with outcomes or events! Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion.
The catheterization lab is activated, but catheterization shows no coronary artery occlusion. ECG shows ST-segment elevation in V3-V6 only with depression in aVR. Initial troponin is mildly elevated. On further questioning, the patient denies recent illness but does mention that her daughter passed away in a car accident yesterday.
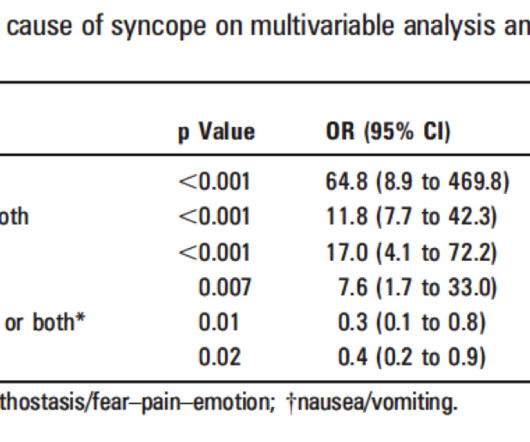
(full text link) Presence of any one of these 8 criteria had 97% sensitivity and specificity of 62% for adverse outcomes: 1) Signs of Acute Coronary Syndrome (ACS), 2) conduction disease, 3) worrisome cardiac history, (eg. The ROSE (Risk Stratification of syncope in the emergencydepartment) Study.
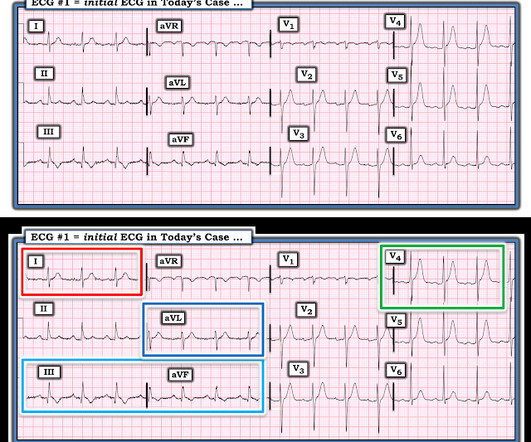
Here is a more detailed history: Presented to the emergencydepartment with chest pain. NEVER diagnose chest discomfort as due to GERD without a coronary workup. Final Thoughts: Dr. Smith instantly recognized that today's initial ECG would clearly be suspicious of a possible acute event, depending on the History.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The following ECG was obtained in the emergencydepartment during active chest pain. He said he had had three episodes of chest pain that day while urinating.
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease. She was discharged again from the emergencydepartment without a second EKG or troponin.
EMS gave aspirin and nitroglycerin, and the patient noted significant improvement on arrival to the EmergencyDepartment. The history in today's case is classic for an acute cardiac event — as this older woman was awakened from sleep by chest pain radiating to her left arm with nausea.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. It may or may not represent early findings in a new acute event. Also : See Ken Grauer's excellent comments at the bottom. EKG 1, 1646: What do you think?
Specifically, patients with SLE face an elevated risk of vascular disease due to higher rates of hypertension and hyperlipidemia, predisposing them to both macrovascular and microvascular events, such as TIA, stroke, and neuropathy (7-9). SLE is considered an atypical risk factor for cardiovascular disease and acute coronary syndrome(8,9,11).
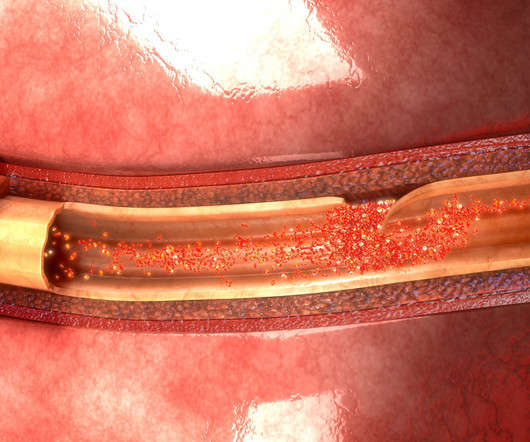
1 It is important to pick up this diagnosis early, as emergency treatment with percutaneous coronary intervention (PCI) to restore blood from to the heart can be lifesaving. TCAD occurs as a result of rapid deceleration, which increases shear forces on the endothelium of the coronary artery.
He presented to the emergencydepartment for evaluation. Rates of occurrence of PIRP have decreased drastically in the era of percutaneous coronary intervention. Incidence and Prognosis of Pericarditis After ST-Elevation Myocardial Infarction (from the Acute Coronary Syndrome Israeli Survey 2000 to 2013 Registry Database).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content