This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Help Support EM Cases by Giving a Donation here: [link] The post EM Quick Hits 59 Traumatic Coronary Artery Dissection, Proper Use of Insulin, Mesenteric Ischemia, Exercise Associated Hyponatremia, AI for OMI appeared first on Emergency Medicine Cases.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023. AEM November 2023.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
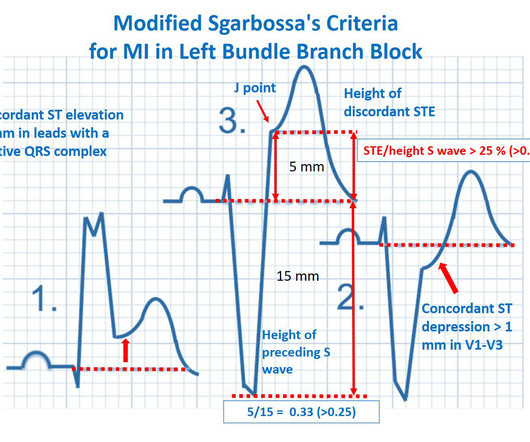
REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion Click here for Direct Download of the Podcast Modified Sgarbossa Criteria deWinters ECG Wellens’ Syndrome STEMI Criteria (Taming of the SRU) Resources REBEL EM: Modified Sgarbossa Criteria: Ready for Primetime?
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. His spouse had called 911 after she heard a loud “thud” in the adjacent room.
Which had a coronary occlusion, and how acute were they? The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion? In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. appeared first on Emergency Medicine Cases.
Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, to consider predisposing (..)
We’ll keep it short, while you keep that EM brain sharp. Upon further research in the 1970’s, retrospective data from autopsies of those patients showed coronary aneurysms 5 Pathophysiology: Kawasaki Disease is a vasculitis of medium sized arteries.
Dodd KW, Elm KD, Dodd EM, Smith SW. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Finally, do a coronary angiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. Heart Rhythm [Internet]. 2014;11:22732277.
ST/T changes: consider the differential including demand ischemia, associated electrolyte abnormalities, Brugada pattern from sodium channel blockade, and acute coronary occlusion vs vasospasm from cocaine. The post ECG Cases 47 – ECG Interpretation in Toxicology appeared first on Emergency Medicine Cases.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Available from: [link] Guldner GT, Smith T, Magee EM.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Hope you’re doing well! How excited would you have been about this case?" No Chest Pain, but somnolent.
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. Lancet Neurol 2009; 8:724-730.
EMS arrived and found him in Ventricular Fibrillation (VF). But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! This patient was witnessed by bystanders to collapse.
Take Home Points: A CCTA is an anatomic test to determine if a patient has normal coronary arteries, non-obstructive disease, or obstructive disease. Take Home Points: A CCTA is an anatomic test to determine if a patient has normal coronary arteries, non-obstructive disease, or obstructive disease.
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. It is spread to V2 and V3.
Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. appeared first on REBEL EM - Emergency Medicine Blog. Excluded: Obvious cause for OHCA prior to SDCT or on hospital arrival. Resus 2023.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
EMS personnel found him seated on a bench, uncomfortable, but without gross distress. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis. He waited for it to subside, but after 30 minutes of persistence he called 911. But the lesion is still active!
Fire/EMS crews found him clammy and uncomfortable. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Learning points 1] Acute Coronary Syndrome has many shades of clinical manifestation.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Here is the LAD after stent placement.
His daughter immediately started CPR and another family member called EMS. When EMS arrived the patient was in ventricular fibrillation. The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. They shocked him twice before return of spontaneous circulation.
EMS finds him supine, alert and oriented, and without any gross distress. Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Crew members note residual pallor and clammy skin. 3] Meyers, H.
Coronary thrombosis is a dynamic process of platelet aggregation and subsequent coagulation. During spontaneous reperfusion -- whether via thrombolysis, or recruitment of collateral circulation -- there exists characteristic ST/T changes on the ECG. Case Review: [link]
PMID: 37634145 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The ECLS-SHOCK Trial: ECPR in Infarct-Related Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog. Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 Control: 9.6%
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. But does this matter? Amsterdam et al. Lupu et al.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
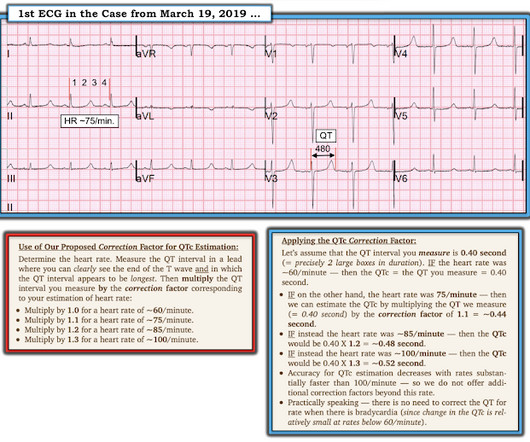
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Clinical Cardiology 2019.
Despite many ECG signs of OMI being missed the door-to-cath time was still fast, because all the healthcare providers were focused on the pathology of acute coronary occlusion and not were distracted by the lack of STEMI criteria. Start using the terms acute coronary occlusion and occlusion MI.
The most likely would be #2) initially normal, then #3) subtle OMI, then #4) obvious STEMI, and then #1) reperfusion: In other words, the patient with an initially normal ECG develops an acute coronary occlusion, with ECGs that progress from subtle to obvious, and then reperfuse after angiography. But that’s not always the case.
Can you identify which ones had acute coronary occlusion? In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. This included the addition several new STEMI equivalents [4] on ECG that warrant “prompt evaluation for emergency coronary angiography.”
Which had acute coronary occlusion? 10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent?
He reported to EMS a medical history of GERD only. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. Cardiology admitted him for observation with plans for next-day coronary angiogram. However, in this context (i.e. 1] Driver, B.
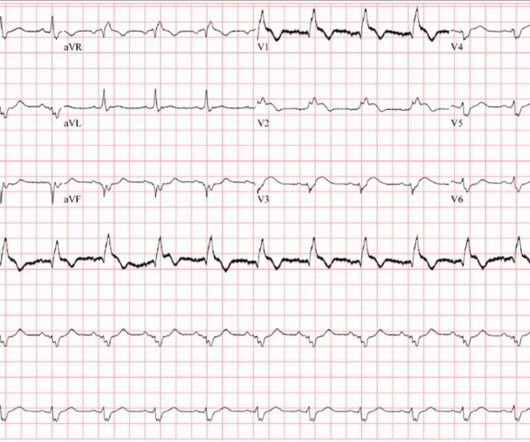
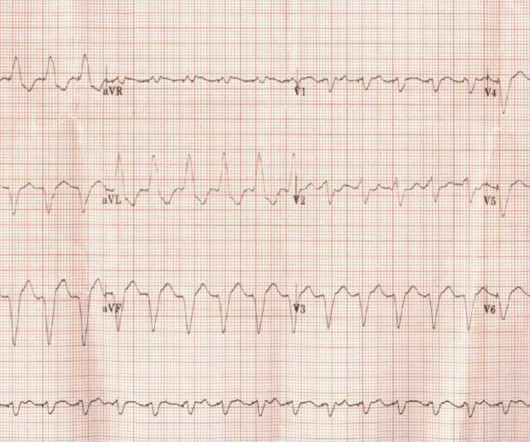
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
Another spurious finding is a QS pattern that mimics Anterior MI, and in the acute setting this may elicit compulsory urge to pursue invasive coronary intervention that is entirely unwarranted. Tom Bouthillet demonstrates appropriate electrode application when capturing the pre-hospital 12 Lead ECG: [link]
Which patients with ECG evidence of coronary occlusion require a CT scan to rule out aortic dissection? What are the range of ECG findings in acute aortic dissection and how do they change management? Dr. Jesse McLaren guides us through 9 cases to answer these and other questions on ECG interpretation in aortic dissection.
This finding should be assumed new, until proven otherwise, during suspected Acute Coronary Syndrome. A possible normal variant is lateral ST elevation (i.e., I/aVL/V5/V6) with bulky T waves when subsequent to a large, slurred S wave. Combination RBBB/LAFB has a high mortality rate in the setting of LAD occlusion.
The Case A 96-year-old female with a history of coronary artery disease, hypertension, and complete heart block status post dual-chamber pacemaker (remote) presents to the ED by EMS with generalized weakness and lethargy.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content