This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
Which had a coronary occlusion, and how acute were they? Jesse McLaren explains 'Late STEMI' and how reperfusion strategies should not be based on time of symptom onset. The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion? appeared first on Emergency Medicine Cases.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Post Created By: William Caputo MD Post Peer Reviewed By: Anand Swaminathan MD, MPH (Twitter @EMSwami ) The post REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion appeared first on REBEL EM - Emergency Medicine Blog.
10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. Which had acute coronary occlusion? The post ECG cases 7: ST elevation in aVR, STEMI-equivalent? Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog.
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial.
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? Now let’s look at the actual sequence, with the addition of clinical context, and see how the patient was managed: The patient received aspirin from EMS and arrived at triage painfree (ECG #1).
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
EMS personnel found him seated on a bench, uncomfortable, but without gross distress. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis. it has been subsequently deemed a STEMI-equivalent. But the lesion is still active!
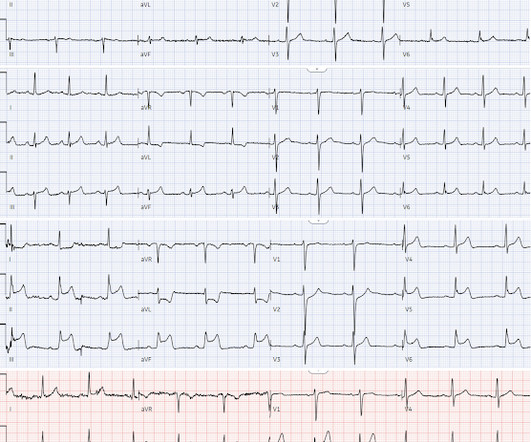
LVH produces secondary repolarization abnormalities that can mimic STEMI. Which had an acute coronary occlusion? Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
Fire/EMS crews found him clammy and uncomfortable. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve.
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. It is spread to V2 and V3.
EMS arrived and found him in Ventricular Fibrillation (VF). But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Cardiac arrest #3: ST depression, Is it STEMI? Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion!
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Clinical Cardiology 2019.
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents. They administer two doses of 10 mg midazolam IM.
He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic. The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand).
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. It’s important to stress the presence of a normal QRS (i.e.,
He reported to EMS a medical history of GERD only. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. However, in this context (i.e.
He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. And the pace only quickens.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" He diagnosed anterior "STEMI" and activated the cath lab. What do you think? But he did well.
When EMS found her, she was dyspneic and diaphoretic. The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography.
EMS was called to evaluate a male patient in his 60s with a chief complaint of chest pain. Onset: Gradual while walking Provoke: Initially the pain felt better with rest Quality: Described as a dull ache Radiate: The pain radiates to the back Severity: 7/10 Time: 3 hours He states that he feels nauseated and vomited x2 prior to EMS arrival.
PMID: 37634145 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The ECLS-SHOCK Trial: ECPR in Infarct-Related Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog. Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 Control: 9.6%
EMS found her acutely ill, mottled, dry mucous membranes, modestly hypotensive, and lethargic. The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Example 1 EMS is called to the residence of an elderly male experiencing profound weakness.
Written by Bobby Nicholson What do you think of this “STEMI”? With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. The patient is unconscious and hypoxic. ng/mL and 0.10
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). Past medical history included HTN, HLD, and MI 10 years prior. link] [1] Zachary et al.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
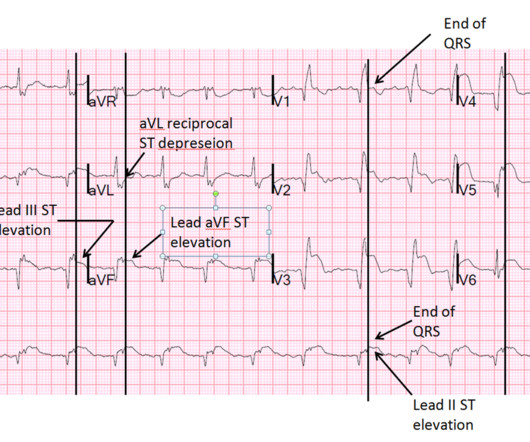
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
EMS arrived and recorded this ECG: What do you think? Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
Jason was very skeptical of STEMI. Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. This also argues against STEMI. He complained of 3 days of diarrhea and abdominal pain.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Serial ECGs enhance the diagnosis of acute coronary syndrome.
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Exact pain history was difficult to ascertain. There was some SOB. Could it be acute (vs.
Generally speaking, right bundle branch block does not mimic, or obscure, the ECG diagnosis of acute STEMI the way left bundle branch block does. Case Review EMS is called to the residence of a 69 y/o M with a chief complaint of chest pain. ECG diagnosis: Borderline sinus bradycardia, 1st degree AVB, RBBB, and occasional PACs.
Can you identify which ones had acute coronary occlusion? In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! At angiogram, there was no change in the coronary arteries. He had no chest pain.
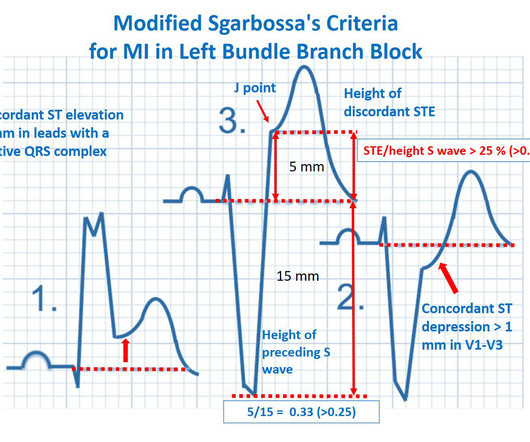
This 74 yo male had just returned to his unit bed after successful PTCA of tight lesions of the first diagonal and obtuse marginal coronaries. There is LBBB with concordant ST elevation in II and aVF (inferior STEMI) and V6 (lateral STEMI); also concordant ST depression in V2 and V3 (Posterior STEMI).
Management must, however, be individualized with respect to the delay to coronary angiography (PCI). TIMI Risk Scores for NSTE-ACS (NSTEMI, UA) and STE-ACS ( STEMI ) can be calculated below. All patients with NSTE-ACS ( NSTEMI or unstable angina) are treated similarly with respect to anti-ischemic and anti-thrombotic drugs.
He had walked into the ED (did not use EMS). Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Exact pain history was difficult to ascertain. There was some SOB.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content