This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. Given no clinical prelude of anginal (or equivalent) descriptors, prior to the acute event, risk stratification of the ECG and Troponin was pursued via Echo and nuclear Myocardial Perfusion Imaging (MPI).
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Furthermore, if this occurs at all, it is a rare event. Unfortunately, vascular remodeling is variable and inconsistent.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? He has no history of coronary artery disease. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022.
Thank you to Dr. Manrique Umana for inviting me and the conference organizers for putting on such an amazing and educational event. Thank you to Dr. Manrique Umana for inviting me and the conference organizers for putting on such an amazing and educational event.
Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial.
This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents. This history immediately places this patient in a high -prevalence population for having an acute event. It's OK not to be certain from the initial ECG as to whether or not an acute event is occurring.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable risk factors for coronary artery disease. In this patient with stuttering symptoms and rising troponin, there is no other option but to perform emergent coronary angiography. Hers is shown below.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. Smith offers the unique perspective of assessing the initial ECG of a patient who has had prior events — and, who now presents with new symptoms. Here is his ED ECG: What do you think?
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. Patient # 1: Assessment of the Initial ECG in the ED … The History for Patient #1 — is clearly concerning for a higher -risk likelihood of having an acute event.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. No ECG was ordered on Day #1.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous. Am Heart J. 2000;139:430–436.
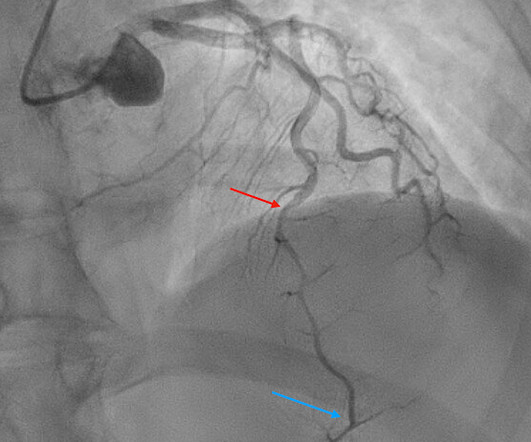
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). They too have dense white masses consistent with coronary atherosclerosis. The blue circle shows the LCx.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
For this reason we did not believe this was an acute coronaryevent and did not activate the cath lab. Here is the troponin profile overnight: This is consistent with cardiac arrest without acute coronary occlusion. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV. Cardiology agreed.
Takeaway lessons * Type B dissections do not involve the heart or coronaries, but Type A vs B nomenclature is falling out of favor versus more anatomically specific labeling; this system helps characterize the gray area between the innominate and the left subclavian. * Find us on Patreon here! Buy your merch here!
This has been to prevent the horrible adverse event called osmotic demyelination syndrome (ODS). There is a high mortality associated with hyponatremia [1-3]. Symptomatic hyponatremia has traditionally been treated with a careful slow continuous infusion of hypertonic saline.
The most likely would be #2) initially normal, then #3) subtle OMI, then #4) obvious STEMI, and then #1) reperfusion: In other words, the patient with an initially normal ECG develops an acute coronary occlusion, with ECGs that progress from subtle to obvious, and then reperfuse after angiography. But that’s not always the case.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. that is, show a pattern of labile ST-T wave changes not due to an acute coronaryevent. I personally can hardly wait for that future version!
Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome? Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. 2016;188(12):E289-E298.
Beats 9-12 : Continuation of the previously described events, all inducible by the pause (and thus, prolongation of refractoriness) created by the PVC of Beat 8. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Beat 4 abruptly halts this repetitious cycle via Peel Back.
Coronaries were clean. Negative serial Troponins were needed to rule out an acute event. If a final test was perceived as "needed" — perhaps a normal coronary CT angiogram could have helped to avoid cardiac catheterization. Sam : "Yes, this case was sent to me. It was a man in his 30s with chest pain.
ST segment elevation, or even an isoelectric ST segment, in these leads is abnormal and should make us concerned for ischemia Source Acute Coronary Occlusion in a Patient With Prior Known Right Bundle Branch Block: Another Chink in the Armor for the ST-Elevation Myocardial Infarction Criteria. Ann Emerg Med. 2023 Aug;82(2):219-221.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion.
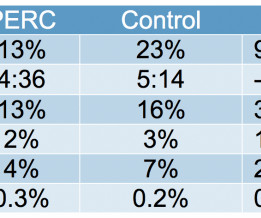
There was no association between moderate to severe chest pain on arrival and major adverse cardiac events at 6 months (20% vs. 14%, p=0.12). Chest pain severity was assessed upon admission to the primary percutaneous coronary intervention hospital. We analyzed 1409 STEMI activations (69% male, 66.3 years old ± 13.7
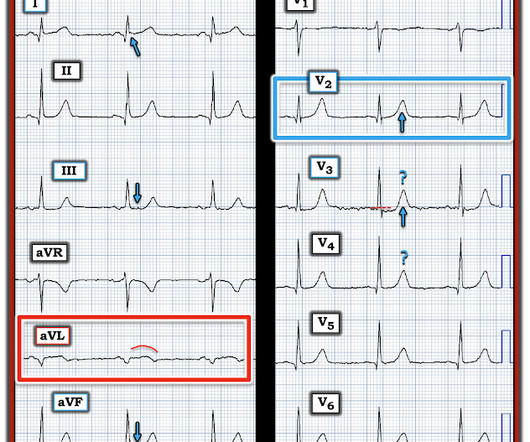
Knowing the patient has a history of coronary disease could be relevant to today's case — as it should add to our suspicion of a new acute event. If this is the case — this size of a Qr wave in lead III, as well as the seemingly wide Q in lead aVF — would seem to suggest prior inferior infarction a t some point in the past.
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Adverse events are common in those using GLP-1 agonists, but the vast majority of these are minor. What are the complications?
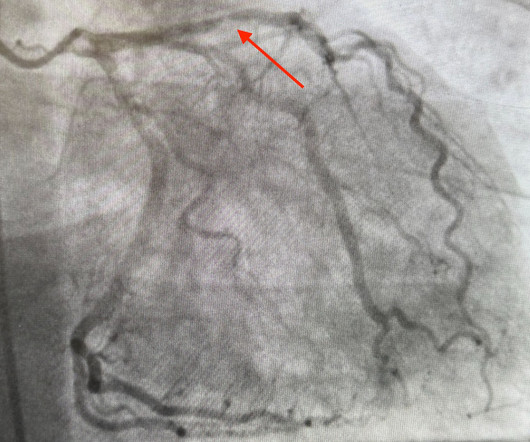
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event. LV Aneurysm vs New Infarction?
All coronary arteries were patent without atherosclerotic change. Dr. Myocarditis can be very difficult to separate from OMI on ECG, and often some form of coronary artery imaging will need to be done to rule out OMI. The ECG shows slight ST Elevation in an inferolateral distribution. Notice how QOH is not fooled by this ST-Elevation.
Takotsubo is a sudden event, not one with crescendo angina. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. Not all patients with acute ( or recent ) MI have chest pain with their event. This does not fit with the clinical scenario in today's case.
have perfect coronary flow by the time of angiogram. The fatter-than-it-should-be T wave in lead aVL is the mirror image opposite picture of the ST-T wave in lead III ==> reciprocal change that strongly suggests a recent ( if not still ongoing acute ) event. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.)
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Impression: In a patient with new symptoms — early repolarization is a diagnosis of exclusion to be made only after you have ruled out the possibility of an acute event.
As discussed above in Dr. Smith's excellent discussion — serial ECGs, correlated to severity of patient symptoms soon confirmed the acute event in today's patient. Once I find 1 or 2 of those leads — closer scrutiny of the remaining 10 leads usually reveals enough abnormalities to support my suspicion.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. Finally, this may just be an incredibly rare event that none of us will ever see again.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardial infarctions. PLUS — Today's patient is an older woman with known severe coronary disease who presented with new chest pain. She's had multiple PCI procedures.
Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 Next day, t he patient was taken for an angiogram and found to have a reperfused LAD lesion with good flow that appeared to the angiographer as if it was a spontaneous coronary artery dissection. She felt more comfortable being admitted.
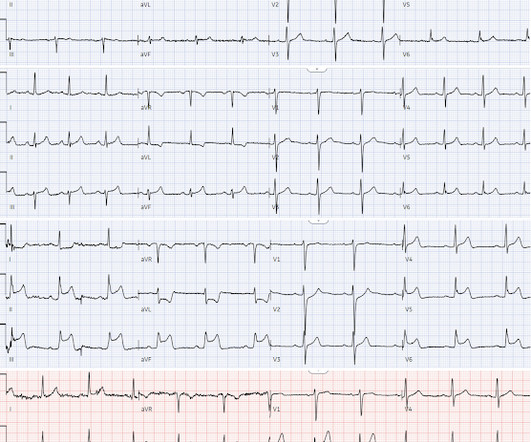
KEY Point: The important distinction that has to be made in today's case, is between ECG findings consistent with this patient's prior LAD OMI — vs — ECG findings of a new acute event superimposed on these prior ECG findings. My "eye" was immediately drawn to leads V1 , V2 , V3 ( within the RED rectangle ).
He subsequently had a syncopal event and was down for 1-2 minutes. The patient had a positive troponin, underwent cath which showed completely clean coronaries, and then underwent EP testing which revealed that, in atrial fibrillation, he has an R-R interval as short as 220 ms, which is dangerously short. His wife called 911.
Summary Indications Prasugrel, in combination with acetylsalicylic acid (ASA), is indicated for the prevention of atherothrombotic events in adult patients with acute coronary syndromes undergoing percutaneous coronary intervention (PCI). – Active bleeding. – Previous stroke or transient ischemic attack.
It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). Prevalence of Total Coronary Occlusion during the Early Hours of Transmural Myocardial Infarction. Akkerhuis KM, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content