This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. CASE CONTINUED She was admitted to the ICU. Finally, do a coronary angiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. but potassium returned normal.
Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Majority of patients had PCI performed (96.6%) Impella CP was most common mechanical circulatory support in patients without ECLS (85.7%) Death From Any Cause at 30d ECLS: 47.8% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 vs 13.9% (RR 0.58; 95% CI 0.33 vs 22.6% (RR 1.03; 95% CI 0.88
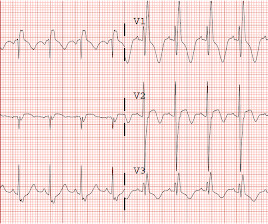
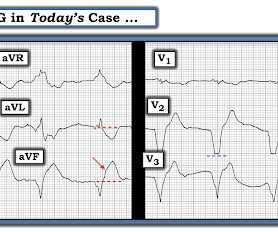
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. In the context of this woman in her 60s who has known coronary disease ( and who is now presenting with acute chest discomfort ) — I interpreted neighboring leads V1 and V2 as part of the same acute process suggested by the QRST in lead V3.
A 65 y/o Female was admitted to the ICU for septic shock. The combination of prolonged QT and deep T wave inversion throughout the precordium is typical of Takotsubo syndrome, or Stress Cardiomyopathy – which can occur in the context of a physiologically distressed ICU patient, further compromising their hemodynamics.
The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care.
Propofol utilized for sedation; patient admitted to ICU for EEG monitoring. NSTEMI dichotomy is not sensitive for true occlusion MI or acute coronary occlusion. “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant miry of patients who have acute coronary occlusion.”
The patient was upgraded to the ICU for closer monitoring. Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. In fact, Kosuge et al. In fact, Kosuge et al. Stein et al. Witting et al. of controls.
The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). Is this: 1. small squares in width (260ms).
Cardiology was consulted, who advised to surveil a metabolic process as this did not strike them as acute coronary syndrome. Thankfully, the patient experienced an uncomplicated ICU stay and subsequently made a full recovery. 2] But there is also Sinus Tachycardia! Such a finding is most dramatic in Lead I, reproduced here.
In ICUs where advanced cerebral monitoring is not in routine use, target an MAP >80 mm Hg unless there are clinical concerns or evidence of adverse consequences (82.6%, 19/23). In ICUs where noninvasive monitoring of cerebral autoregulation is in routine use, maintain MAP at or near the predicted MAPOPT (88.2%, 15/17).
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. We’ll keep it short, while you keep that EM brain sharp. Vital signs include BP 90/48, HR 122, T 98.3
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Instead — it commonly reflects ischemia from severe underlying coronary disease. QTc/QUc is in the range of 630 msec. See these other relevant cases: What are these bizarre bigeminal PVCs??
Clinical Question : In patients who suffer an OHCA without ST-segment elevation on the post-resuscitation ECG, will early coronary angiogram (CAG) vs. delayed CAG improve outcomes? Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial.
He was admitted to the ICU and was unstable, in shock, overnight. If the situation is not right for acute coronary occlusion, then the ECG findings probably do not represent acute coronary occlusion. Despite the eye-catching ST-T wave changes that came-and-went a number of times — there was no acute coronary occlusion.
The TEG group had a shorter ICU length of stay in the first admission. Patients exclusively managed in the ICU which decreases applicability for patients in other locations Very small sample size of 96 patients No definition was provided for exclusion criteria of significant cardiopulmonary disease.
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. More commonly, however, ECG and/or echo wall motion abnormalities are due to pre-existing disease, especially coronary disease complicating trauma. She was intubated.
Electrocardiographic diagnosis of acute coronary Occlusion Myocardial Infarction in ventricular paced rhythm using the modified Sgarbossa criteria. There is no doubt about these 2 EKGs: they are due to acute coronary occlusion. He went into cardiogenic shock and is intubated in the cardiac ICU. Annals of Emergency Medicine 2021.
Liberal O2 (PaO2 13 to 14kPa (98 to 105mmHg) Initial FiO2 set at 0.6 Liberal O2: 33.9% HR 0.95; 95% CI 0.75 to 1.21; p = 0.69 Results were consistent in all prespecified subgroups Death at 90d Restrictive O2: 28.7% Liberal O2: 31.1% HR 0.93; 95% CI 0.72 Higher MAP: 34.0% HR 1.08; 95% CI 0.84 to 1.37; p = 0.56 Liberal O2: 33.9% HR 0.95; 95% CI 0.75
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. We’ll keep it short, while you keep that EM brain sharp. Symptoms may range from days to months prior to stroke onset.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Interventions during the acute phase of treatment post return of spontaneous circulation (ROSC) are therefore critical.
When it’s too low the oveerall CO is too low, at some point it’s too fast, impairing cardiac and coronary filling and hence impairing stroke volume. Pretty much all vasoactive medications have the same end point – that is the release, utilisation or sequestration of intracellular calcium.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels. Increases coronary blood flow. Coronary flow enhanced.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. No history of GIB, dysuria, or GU symptoms. mg/dL, K 3.5
Wellens pattern is a term which refers to coronary reperfusion morphology in the anterior leads) The best answer is because the entire gestalt of the ECG shows acute right heart strain instead, and just does not look like Wellens after you've seen Wellens hundreds of times. Why is it not Wellens??? She was discharged and did well.
If she had no risk factors, it is doubtful that she would have developed such extensive coronary artery disease as we see on the angiogram. I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. These look like ischemic ST segments and T-waves.
This vasoconstriction affects pretty much all the vasculature including things like the coronaries (not so good) but does seem to spare the pulmonary arteries meaning it may be good in those with pulmonary hypertension. How does it work? Well this is where the fun beings. What other receptors is it worth knowing about? How does it work?
in the ICU but survived with excellent function. Several hours prior to presentation, while driving his truck, he started experiencing new central chest pain, without radiation, aggravating/alleviating factors, or other associated symptoms. You diagnose pericarditis at your peril! Acute MI is frequently misdiagnosed as pericarditis.
If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training. The patient did well. Patel et al., Krucoff et al.) Patel et al. American Journal of Cardiology 1990.
Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Acute coronary syndrome is unlikely to be one of those entities. Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient.
Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His troponin I peaked at 97 ng/mL (very large MI!). His follow up ECHO the next day revealed an EF of 24% and a posterior wall motion abnormality. Herzog et al. What can we learn?
A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid. There are too-numerous-to-count cases on Dr. Smiths ECG Blog in which emergency providers diagnosed acute pericarditis that was really acute coronary syndrome.
3,10 Coronary Allograft Vasculopathy Nicknamed “The Achilles Heel of Heart Transplantation,” this accounts for the majority of patient mortality in the 5-10 year range. 10 It affects the whole length of the vessel and all layers of the coronary vasculature rather than just the intima, which is seen in non-transplant atherosclerosis.
Some of the critical differentials include pulmonary embolism, acute decompensated heart failure, pneumonia, pneumothorax, and acute coronary syndrome. Anginal chest pain, chest heaviness, or evidence of fluid overload suggest acute coronary syndrome or acute decompensated heart failure. Signs and symptoms of systemic infection (e.g.,
Fifth , potential management actions are in your hands; you do not need to request a coronary interventionalist or cath lab team. She was critically ill and required noninvasive positive pressure ventilation and ICU admission for suspected infectious respiratory illness. Sinus tach is often misinterpreted as a dysrhythmia.
He was started appropriately on vancomycin and cefepime and accepted for ICU admission but remains in the ED due to boarding and bed lock. Left ventricular outflow tract obstruction in ICU patients. He has clinically deteriorated and required intubation. m/s)—problematic and elevated > 50 mm Hg (2.5 Curr Opin Crit Care.
The ultimate goal is to optimize coronary perfusion pressure (CPP)—in other words, the amount of blood flow into the coronary arteries. LVEDP (measured in the ICU using a Swan-Ganz or pulmonary artery catheter) is the pressure inside the left ventricle at the end of diastole, when the LV is at its fullest. So how do we treat it?
This is likely because Dexmed helps dampen the sympathetic response to perioperative stress, improving coronary artery perfusion. Dexmedetomidine is currently licensed only for adult sedation in an ICU setting, but guidelines exist to support its off-licence use in paediatric intensive care (PICU).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content