This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
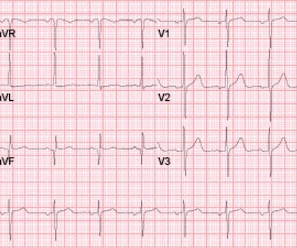
Propofol utilized for sedation; patient admitted to ICU for EEG monitoring. Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4.
Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Majority of patients had PCI performed (96.6%) Impella CP was most common mechanical circulatory support in patients without ECLS (85.7%) Death From Any Cause at 30d ECLS: 47.8% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 vs 13.9% (RR 0.58; 95% CI 0.33 vs 22.6% (RR 1.03; 95% CI 0.88
Subtle as a STEMI." (i.e., A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Cardiology was consulted, who advised to surveil a metabolic process as this did not strike them as acute coronary syndrome. Closer inspection will show that it is Sinus, after all.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." The patient was upgraded to the ICU for closer monitoring. If this EKG were handed to you to screen from triage without any clinical information, what would you think? In fact, Kosuge et al.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Is it STEMI? Instead — it commonly reflects ischemia from severe underlying coronary disease. See these other relevant cases: What are these bizarre bigeminal PVCs?? Chest pain in high risk patient.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial. Statements: In ICUs where advanced cerebral monitoring is not in routine use, target an MAP >80 mm Hg unless there are clinical concerns or evidence of adverse consequences (82.6%, 19/23).
If she had no risk factors, it is doubtful that she would have developed such extensive coronary artery disease as we see on the angiogram. I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Her repeat ECHO showed an improving EF of 37%.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. Lupu L, et al. mg/dL, K 3.5
in the ICU but survived with excellent function. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs.
Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His troponin I peaked at 97 ng/mL (very large MI!). His follow up ECHO the next day revealed an EF of 24% and a posterior wall motion abnormality. Herzog et al.
A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid. There are too-numerous-to-count cases on Dr. Smiths ECG Blog in which emergency providers diagnosed acute pericarditis that was really acute coronary syndrome.
He was started appropriately on vancomycin and cefepime and accepted for ICU admission but remains in the ED due to boarding and bed lock. Left ventricular outflow tract obstruction in ICU patients. He has clinically deteriorated and required intubation. m/s)—problematic and elevated > 50 mm Hg (2.5 Curr Opin Crit Care.
In the EMS setting, the most common cardiogenic shock patient is most likely a STEMI. The ultimate goal is to optimize coronary perfusion pressure (CPP)—in other words, the amount of blood flow into the coronary arteries. When the heart is full, it puts pressure on the myocardium, compressing the coronary microvasculature.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content