This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. She does not smoke.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. The patient is a 75-year old man with known coronary disease, including prior LAD and LCx OMI. That this patient has severe underlying coronary disease is indisputable.
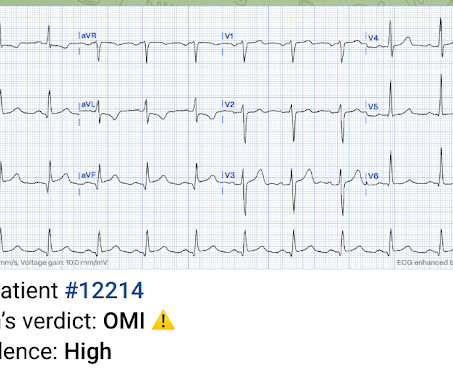
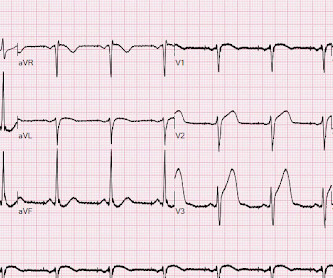
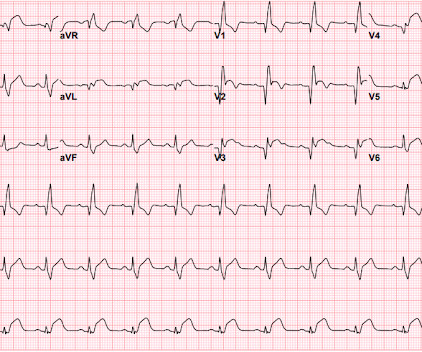
This ECG was texted to me with no other information. I assumed the presentation was consistent with acute MI. What did I say? Activate the cath lab." The T-waves in V2-V6 are diagnostic. It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. There is also some non-diagnostic STE in inferior leads.
Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. Design: Prospective, observational, before and after implementation of a protocol study. Known cardiac defibrillator. Pre-existing DNR order.
Studies have shown that oxygen can cause vasoconstriction, increase blood pressure and decrease coronary artery blood flow ( Kones et al AM J Med 2011). They felt this would help inform guideline writers on making recommendations in this area. What would you rather have, more death or less VT? Class IIb, LOE C-LD)
Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Majority of patients had PCI performed (96.6%) Impella CP was most common mechanical circulatory support in patients without ECLS (85.7%) Death From Any Cause at 30d ECLS: 47.8% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 vs 13.9% (RR 0.58; 95% CI 0.33 vs 22.6% (RR 1.03; 95% CI 0.88
An 86-year-old man with a past medical history of coronary artery disease, hypertension, hyperlipidemia, chronic kidney disease, COPD, choledocholithiasis requiring ERCP and sphincterotomy 2 years ago presented with five days of feeling unwell. History was limited due to cognitive impairment. He denied changes to urination or bowel movements.
Past medical history includes coronary stenting 17 years prior. This was shown to me with no clinical information and I said "It is VT until proven otherwise." Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Initial ED ECG: What do you think?
What would you do at this time with this information? But pain is an important signal in MI and informs the clinician of the urgency. For the same reason, you should not delay coronary angiography because pain resolves with morphine. So I would be worried about inferior OMI. A patient with OMI can have a totally normal ECG!"
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. This included the addition several new STEMI equivalents [4] on ECG that warrant “prompt evaluation for emergency coronary angiography.”
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI".
A 50-year-old Caucasian female with a history of hypertension, coronary artery disease, and insulin-dependent diabetes mellitus presents to the emergency department with a complaint of painful sores on the top of her left foot. View other cases from this Clinical Image Series on ALiEM.
Caring for critically ill patients with limited information requires snap assessments and judgements for timely resuscitation and efficient emergency department throughput. In the age of big data, more information sounds like a boon. With what I can only describe as a “grimace” by a singular word, his face conveyed so much more.
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. But STEMI criteria is only 43% sensitive for OMI.[1] De Alencar Neto.
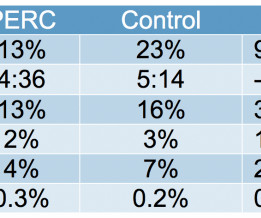
Listen to the podcast on iTunes to hear Dr. Kline discuss some background information on the diagnosing of pulmonary embolism and the PERC Rule. * The eight-items include the following clinical criteria. If the answer to any of these questions is positive a d-dimer is indicated.
But do they represent acute coronary occlusion? But coronaries were normal, and serial high sensitivity troponin was undetectable. Based on ECG changes and echo findings, the patient was diagnosed as coronary vasospasm. I sent both ECGs to Dr. Smith, with the only information that these were prior vs new ECG.
At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD
This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. Coronaries were clean. If a final test was perceived as "needed" — perhaps a normal coronary CT angiogram could have helped to avoid cardiac catheterization. I assumed it was a patient with acute chest pain. What do you think, Steve? Real or just fake?"
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. If so, how will they change management?
If this EKG were handed to you to screen from triage without any clinical information, what would you think? Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. What do you think? In fact, Kosuge et al. Accessed May 28, 2024. Stein et al.
Accompanying the ECGs is some clinical information. Look at the ECGs and consider the timeline and other information. Would you change you interpretation if the following information was added? B elow are 4 ECGs from the same patient. At the bottom will be five alternative clinical scenarios to explain the findings.
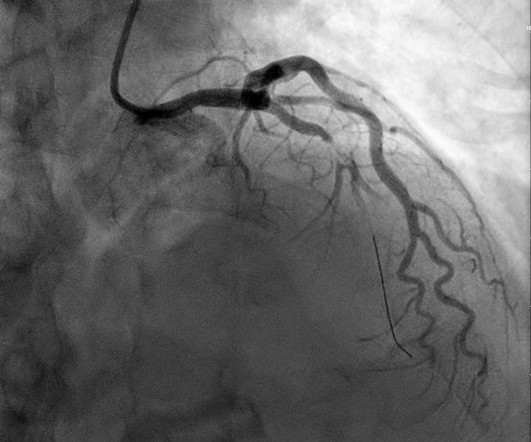
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
I read this blinded, with no clinical information, and read it as inferior OMI. The Queen of Hearts interprets it blinded also (no clinical information and no previous ECGs or serial ECGs). A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion. Deutch et al.
ST segment elevation, or even an isoelectric ST segment, in these leads is abnormal and should make us concerned for ischemia Source Acute Coronary Occlusion in a Patient With Prior Known Right Bundle Branch Block: Another Chink in the Armor for the ST-Elevation Myocardial Infarction Criteria. Ann Emerg Med. 2023 Aug;82(2):219-221.
I sent the top ECG to Dr Smith with no information and without the baseline ECG. The patient was referred for coronary angiography which did not reveal any atherosclerotic changes. A formal echo at the PCI center after coronary angiography revealed a large septal and apical WMA. The chest pain quickly subsided.
Written by Pendell Meyers I was reading ECGs in a database (without any clinical information) when I came to this one: What do you think? For clarity in Figure-1 — I've reproduced the initial ECG that was shown above in today's case, which Dr. Meyers ventured to read without the benefit of any clinical information.
Written by Pendell Meyers Both of these cases were sent to me with no information other than adults with acute chest pain. What would be your response? Case 1: Case 2: What if I told you that Case 1 has an abnormal initial troponin, and Case 2 has a normal initial troponin? Case 1 An elderly male presented with chest pain. What a farce.
Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. STE at 60 ms after the J-point is substantially higher than at the J-point.
As crude measures they fail to incorporate any other information into their estimates, including potential confounders for the relationship between the test result and the outcome. Sensitivity and Specificity are crude metrics, meaning they only look at the effect of a single measure and a single outcome.
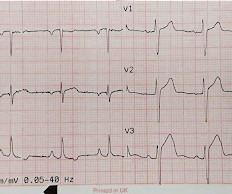
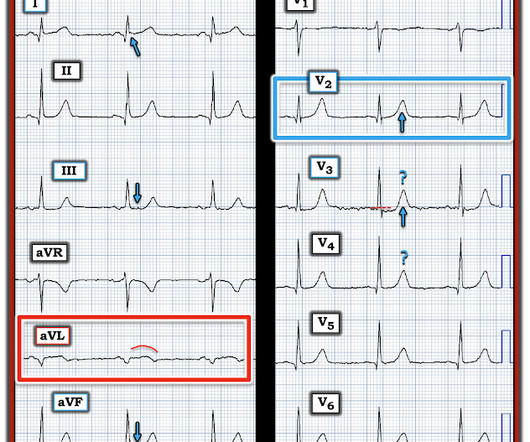
Clearly, more information is needed before a definite decision can be reached — but the “onus of proof” is on the clinician to rule out acute LAD occlusion. There is a small amount of STE in V2 and V3, with a very small amount of STD in V4-V6. The T-waves are not definitively hyperacute. There was no prior for comparison.
The chest pain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. EMS arrived and recorded this ECG: What do you think?
Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. If you have a story to share click here. Who is responsible for notifying patients of post discharge findings?
Learning points: Both patients and other medical providers can report confusing and often contradictory information that obfuscates the diagnosis (in this case, WPW). Serial ECGs enhance the diagnosis of acute coronary syndrome. This can occur due to scar ( e.g. post infarct VT) or anatomical variants ( e.g. AVNRT or AVRT). Washam, J.
All coronary arteries were patent without atherosclerotic change. Dr. Myocarditis can be very difficult to separate from OMI on ECG, and often some form of coronary artery imaging will need to be done to rule out OMI. In any case, the ECG is diagnostic of severe ischemia and probably OMI. Concordant STE of 1 mm in just one lead or 2a.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardial infarctions. Do you need to get more information? She's had multiple PCI procedures. The question is, does she need to go urgently to the cath lab or can she wait.
Distilling this case into its most salient components, a man with multiple risk factors for coronary disease is presenting with several days of chest pain and markedly elevated troponin with no other reason to explain the lab abnormality ( e.g. sepsis). High sensitivity troponin I (hsTnI) obtained around that time was 5548 ng/L (ref. <
Clinical Question : In patients who suffer an OHCA without ST-segment elevation on the post-resuscitation ECG, will early coronary angiogram (CAG) vs. delayed CAG improve outcomes? Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial.
Today's CASE: We have only been provided with limited information about the patient in today's case — namely, that is a middle-aged adult who presented with CP ( C hest P ain ). Knowing the patient has a history of coronary disease could be relevant to today's case — as it should add to our suspicion of a new acute event.
Any ST Depression Maximal in V1-V4 is OMI until proven otherwise I sent this ECG with no information to Pendell. have perfect coronary flow by the time of angiogram. The large upright T-wave in V2 is consistent with reperfusion. We send each other EKG by the dozens every day. Most are OMI look alikes (mimics).
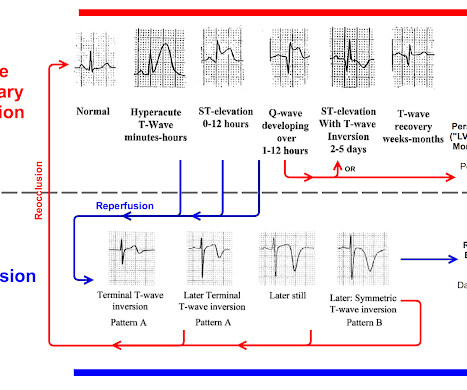
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. that is, show a pattern of labile ST-T wave changes not due to an acute coronary event. I personally can hardly wait for that future version! Learning Point: 1.
This was sent to me with no information and I immediately replied that it was diagnostic of LAD OMI. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chest pain. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus.
Just so you know this ECG interpretation is not done by the retrospectoscope: I sent it to Dr. Smith without any information, and he immediately responded: "Infero-postero-lateral OMI" The ECG had a computer and final cardiology interpretation of “possible inferior infarct, age undetermined”, because of Q waves.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content