
ECG Cases 45 ECG in Weakness and Neurological Symptoms
Emergency Medicine Cases
SEPTEMBER 12, 2023
The post ECG Cases 45 ECG in Weakness and Neurological Symptoms appeared first on Emergency Medicine Cases.
Emergency Medicine Cases
SEPTEMBER 12, 2023
The post ECG Cases 45 ECG in Weakness and Neurological Symptoms appeared first on Emergency Medicine Cases.

Dr. Smith's ECG Blog
SEPTEMBER 18, 2024
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Thus, the lumen observed may actually still be the same size as the original, normal lumen. Unfortunately, vascular remodeling is variable and inconsistent.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.

Emergency Medicine Cases
FEBRUARY 28, 2023
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.

ACEP Now
DECEMBER 6, 2024
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.

The Skeptics' Guide to EM
NOVEMBER 25, 2023
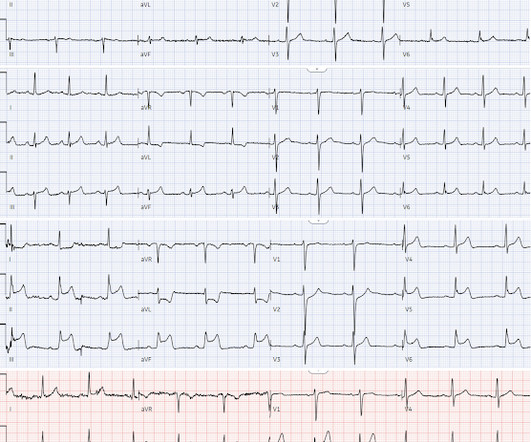
A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital. Background: We have covered the issue of heart attacks several times on the SGEM. Reference: Stopyra et al.

EMS 12-Lead
APRIL 9, 2024
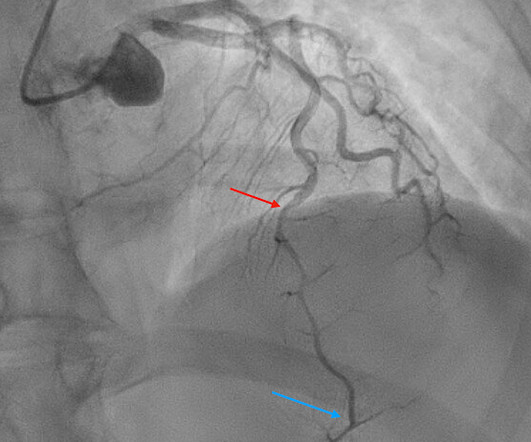
There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. 2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. He awoke earlier that morning in his usual state of health. Type I ischemia.
Emergency Medicine Cases
DECEMBER 16, 2019
Which had acute coronary occlusion? In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI. The post ECG Cases 4: Lateral STEMI or Occlusion MI?

Expert insights. Personalized for you.
































Let's personalize your content