

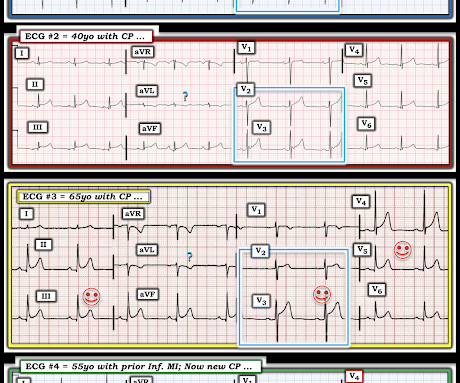
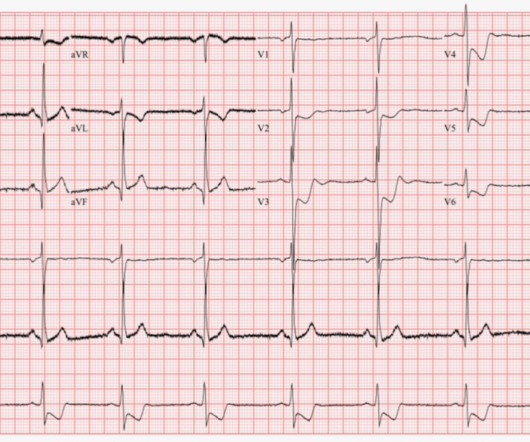
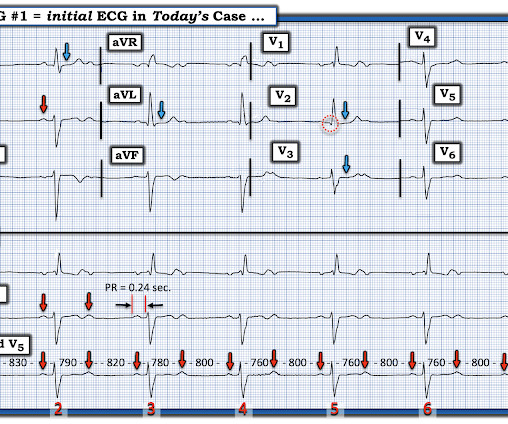
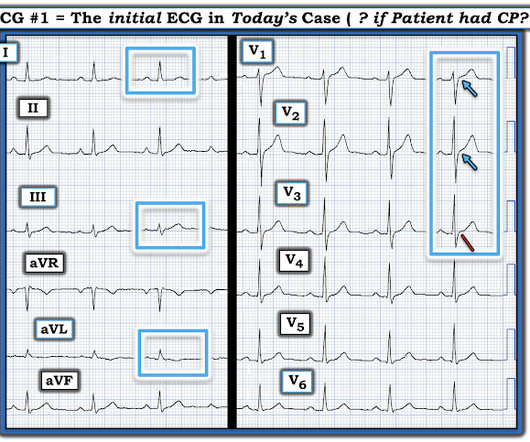
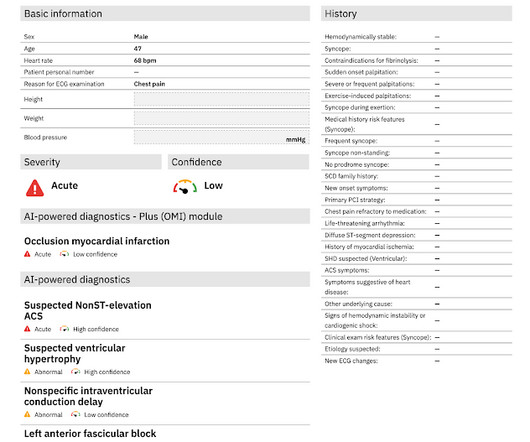
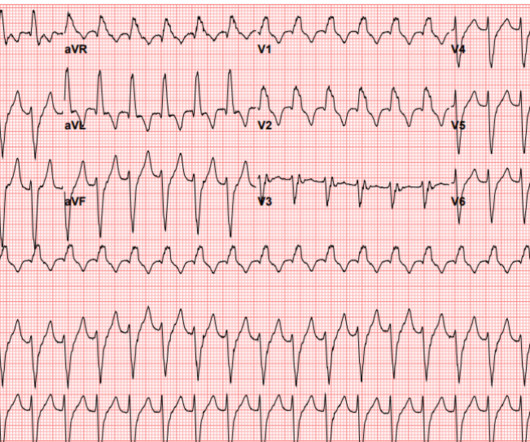
Dynamic OMI ECG. Negative trops and negative angiogram does not rule out coronary ischemia or ACS.
Dr. Smith's ECG Blog
SEPTEMBER 18, 2024
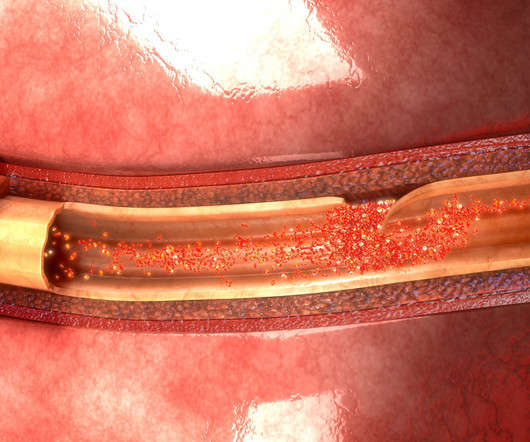
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Thus, the lumen observed may actually still be the same size as the original, normal lumen. Unfortunately, vascular remodeling is variable and inconsistent.


































Let's personalize your content