This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 20-something presented after a huge verapamil overdose in cardiogenic shock. And she does not know that this is an overdose; she thinks it is a patient with chest pain!! Comment on High Dose Insulin and Calcium Channel Blocker Overdose I do not have any explanation for the ST-T abnormalities here. The initial K was 3.0
ST/T changes: consider the differential including demand ischemia, associated electrolyte abnormalities, Brugada pattern from sodium channel blockade, and acute coronary occlusion vs vasospasm from cocaine. The post ECG Cases 47 – ECG Interpretation in Toxicology appeared first on Emergency Medicine Cases.
Opioid overdose remains the leading cause of cardiac arrest due to poisoning in North America. Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association 2023 Guideline for managing cardiac arrest or life-threatening toxicity due to poisoning was recently released. Top 10 Take Home Pearls 1.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! It also does not uniformly indicate severe coronary disease. The ECG shows severe ischemia, possibly posterior OMI.
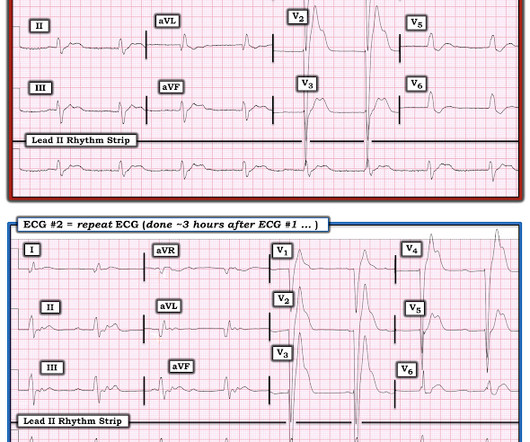
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. which would suggest reduced rates of major adverse cardiac events with coronary artery bypass grafting." On the other hand, stable EKG over an hour in the setting of ongoing acute coronary syndrome is again unusual.
Calcium is associated with harm but is still necessary in certain situations (hyperkalemia, calcium channel blocker overdose) (Level 3 recommendation: no benefit). Major Updates Avoid routine use of calcium in patients with cardiac arrest. COR 2a, LOE B-R. COR 2a, LOE C-LD. COR 2b, LOE B-R. COR 2b, LOE B-R. COR 3, No benefit, LOE B-R.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
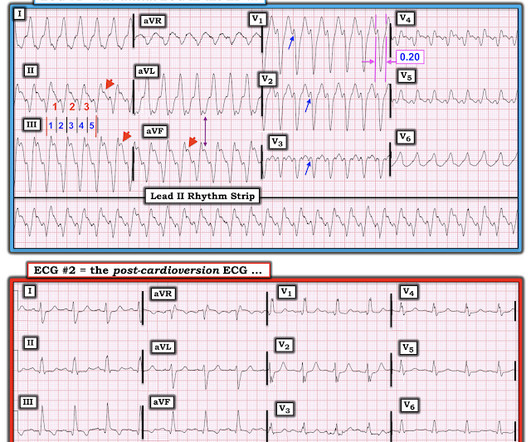
A New Seizure in a Healthy 20-something More cases of long QT not measured correctly by computer (these are all fascinating ECGs/cases): Bupropion Overdose Followed by Cardiac Arrest and, Later, ST Elevation. Instead — it commonly reflects ischemia from severe underlying coronary disease. QTc/QUc is in the range of 630 msec.
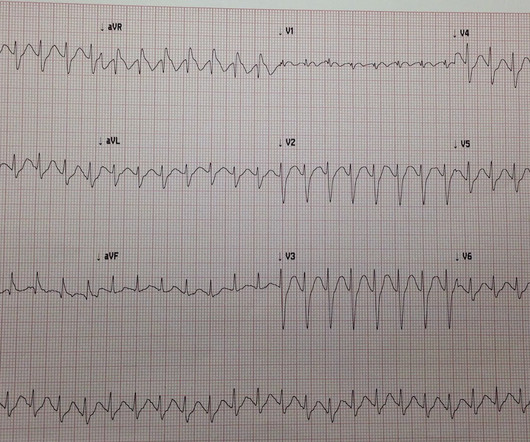
Common culprits in this situation are tricyclic overdose and cocaine toxicity (remember cocaine not only increases dopamine in central synapses, but is also a local anesthetic (-caine!) I could barely see them in lead II: There are probable P-waves at the arrows, but I wasn't certain I texted back: "Could be very fast sinus." Monitor Lead I.
An elderly woman with history of coronary disease presented with CP and SOB and hypotension by EMS. Angiogram: Severe coronary artery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronary artery disease.
Upwardly Concave ST Segment Morphology Is Common in Acute Left Anterior Descending Coronary Artery Occlusion. Paper published: Terminal QRS distortion not found in any ECG of Early Repolarization TQRSD is defined as the absence of BOTH an S-wave and a J-wave in leads V2 or V3. 2 comments : 1. Journal of Emergency Medicine 2006; 31(1):67-77.
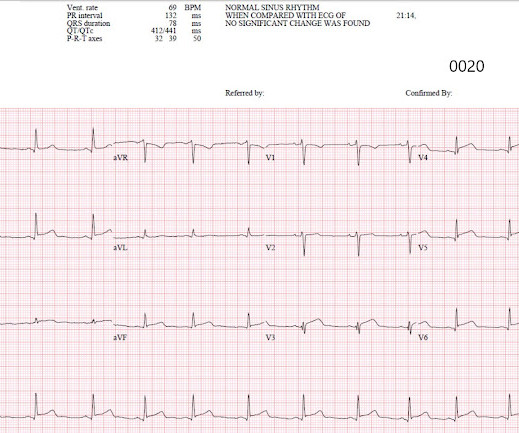
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content