This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Paramedics provided another 3 sprays of nitro, and 6mg of morphine, which reduced but did not resolve the pain. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. of such ‘high risk Non-STEMI’ patients get angiography within 2 hours.[2] But does this matter?
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (Ret) @DidlakeDW Expert contribution by Dr Robert Herman @RobertHermanMD @PowerfulMedical (Chief Medical Officer) An adult male called 911 for new-onset epigastric burning. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
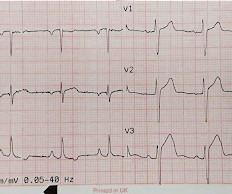
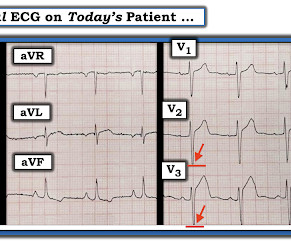
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. In isolation this ECG does not show OMI, but following the paramedic ECGs this indicates spontaneous LAD reperfusion.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
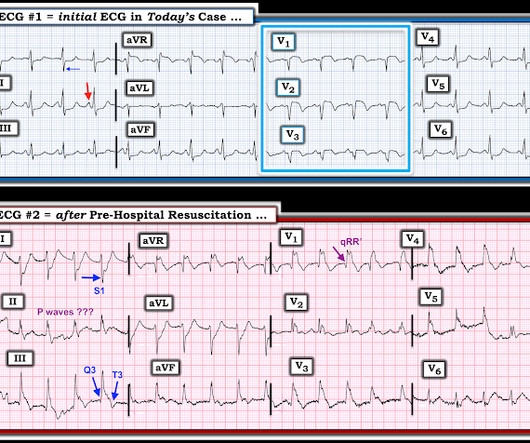
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. EMS arrives and finds the patient in monomorphic ventricular tachycardic (VT) cardiac arrest.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. Are these findings consistent with a particular coronary distribution?
But they have an interest in ECGs, lots of exposure to OMI ECGs as well as normals and mimics, an interest in acute coronary occlusion, and a talent for seeing the subtle waveform findings of acute OMI. He was a paramedic at the time. Such proficient interpreters include health care assistants and EKG technicians.
Madden, Paramedic. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). An interesting comment provided by Paramedic Madden is that a few team members initially interpreted the T wave presentation as hyperkalemia, as opposed to occlusive hyperacuity. Physiology.
The ECG is determined to be non-diagnostic by the treating paramedic. The treating paramedic withholds aspirin. At the hospital a 12-lead ECG is recorded within 10 minutes and read by the attending physician, who activates the “Code STEMI” protocol. The paramedic, feeling a bit sheepish, asked me to review the case.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Written by Jesse McLaren Two 70 year olds had acute chest pain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. Who needs the cath lab?
Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Vitals were normal.
Jason was very skeptical of STEMI. Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. This also argues against STEMI. He complained of 3 days of diarrhea and abdominal pain.
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. He had a prehospital ECG.
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. She went to angio and had normal coronaries. Paramedics found her semi-conscious, pale, cool, diaphoretic, tachypneic, very hypotensive. Medics recorded the above ECG and called a STEMI alert. Her troponin I returned at 900 ng/L.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. One need not have obstructive coronary disease to have occlusive thrombus!
This case was sent by Lou B, a paramedic and RN. Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 Pattern looked to be BER.
The paramedic recorded a series of ECGs; the initial ECG is representative here: Computer read: “ Normal ECG ” What do you think? The paramedic interpreted this as a STEMI. Can you employ the Subtle Anterior STEMI calculator ? It is not yet available, but this is your way to get on the list. or LAD occlusion?
Jason was very skeptical of STEMI. Pretest probability: Especially when there is no Chest pain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear. This also argues against STEMI. He complained of 3 days of diarrhea and abdominal pain.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Look at the aortic outflow tract.
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI. In any case, these further support the diagnosis of coronary occlusion or near occlusion.
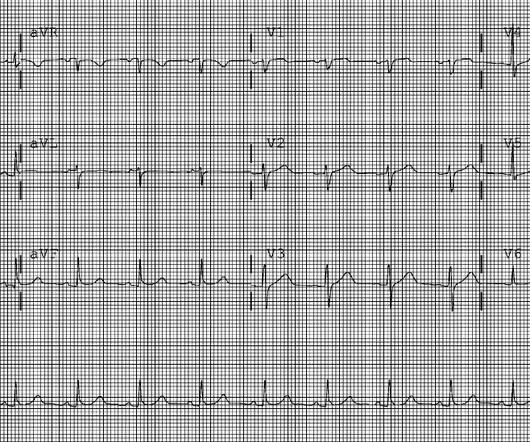
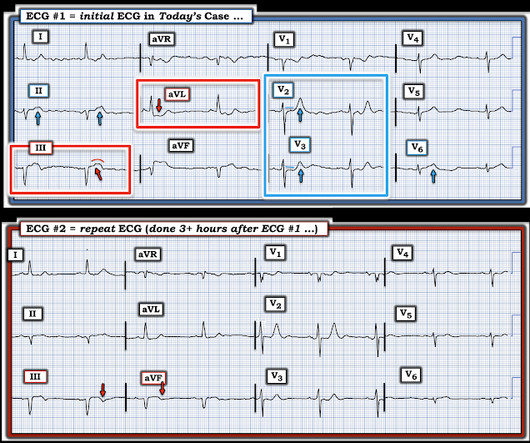
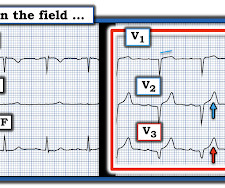
Her initial 12-lead ECG that was obtained by paramedics in the field is shown in Figure-1. Figure-1: The initial ECG in todays case, obtained by paramedics in the field. ( NOTE: Because LBBB changes the sequence of LV repolarization it may be more difficult to recognize acute coronary occlusion on ECG. See text ). ( See text ).
The paramedics found the patient with ROSC and a GCS 7, and an ECG showing LBBB with possible lateral ST elevation. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. This ALONE is very strong evidence of acute coronary occlusion. Any indications for cath lab activation?
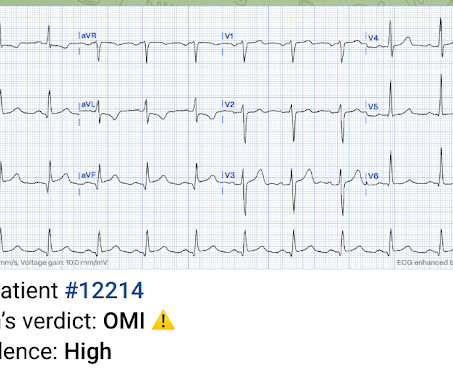
Here’s the paramedic ECG (digitized by PMcardio). STEMI negative : the EMS automated interpretation read, “STEMI negative. But the latest ACC consensus on the evaluation of chest pain in the ED warns that “STEMI criteria will miss a significant minority of patients with acute coronary occlusion.”[1]
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. 1] Here is the admitting ED ECG after cancellation of Code STEMI. 1] Driver, B.
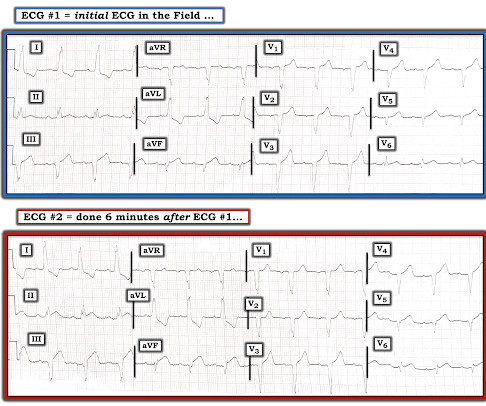
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic @DidlakeDW A 50 y/o Male was taking his dog for a leisurely stroll through the park when he suddenly experienced new onset chest discomfort. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGBlog An adult female called 911 for chest discomfort and difficulty breathing. Cardiology was consulted, who advised to surveil a metabolic process as this did not strike them as acute coronary syndrome.
When the paramedics arrived, they obtained a 12 lead ECG and confirmed the unstable vital signs. There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI).
This was shown to me by a very astute Hennepin paramedic. Although this comes from a Hennepin paramedic, the patient was not brought to Hennepin County Medical Center. It is important for cardiologists to realize that a paramedic may see something they do not. of this post. This is my reponse. This is not tribalism.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. STEMI criteria are only 43% sensitive for OMI.
Background: Patients with ST-elevation myocardial infarction (STEMI) in regional Tasmania frequently encounter reperfusion delays. This study aimed to describe a cohort of the first patient encounters involving STEMI treated under the new guideline to review the implications of the PHT initiative and inform ongoing implementation.
She was found by paramedics with an oxygen saturation of 64%, but could not tolerate BiPAP during transport due to claustrophobia. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI. Management?
You’re me, and you’re in paramedic school, in the thick of the cardiology section. In the EMS setting, the most common cardiogenic shock patient is most likely a STEMI. The ultimate goal is to optimize coronary perfusion pressure (CPP)—in other words, the amount of blood flow into the coronary arteries.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. Lidocaine had been used for the prevention of VF since the 1960s after coronary care units became a standard setting for the treatment of AMI.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, when someone has immediate resuscitation of an arrest witnessed by paramedics, they rarely have a GCS of 3 (deep coma).
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chest pain that started while working at his desk. The paramedic thought it was LAD OMI, but wasn't certain. The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". Pain was decreased to 2/10.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. So even a massive STEMI, if it reperfused quickly, can result in a relatvely low troponin (in contrast to the next case!) Wehrens XH, Doevendans PA, Ophuis TJ, Wellens HJ.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content