This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
You continue with compressions and defibrillations and your partner places an advanced airway. SGEM#143: Call Me Maybe for Bystander CPR * SGEM#152: Movin’ on Up – Higher Floors, Lower Survival for OHCA * SGEM#162: Not Stayin’ Alive More Often with Amiodarone or Lidocaine in OHCA * SGEM#189: Bring Me to Life in OHCA *
The post Ep 169 Cardiac Arrest Controversies – Chest Compressions, Dual Defibrillation, Medications and Airway appeared first on Emergency Medicine Cases.
Case: You are the Chief of your local Fire and EMS Department, and an individual contacts you saying […] The post SGEM#380: OHCAs Happen and You’re Head Over Heels – Head Elevated During CPR? first appeared on The Skeptics Guide to Emergency Medicine. Date: October 18th, 2022 Reference: Moore et al.
Defibrillation Strategies for Refractory Ventricular Fibrillation. Defibrillation Strategies for Refractory Ventricular Fibrillation. He has been an ACLS instructor for close to 30 years and notably his first publication focused on out-of-hospital defibrillation. Defibrillation Strategies for Refractory Ventricular Fibrillation.
We should focus more on high-quality CPR and early defibrillation for shockable rhythms and less on type of supraglottic airway device. The SGEM has also covered prehospital intubation using supraglottic devices for out-of-hospital cardiac arrests (OCHAs) with PA Missy Carter ( SGEM#247 and SGEM#396 ).
This is because of the ease of finding anatomic landmarks and their location away from other procedures like defibrillation, CPR, and airway management. The classic location for IO placement is the tibial plateau.
You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive. Unfortunately, most patients don’t receive these crucial interventions.
In this CritCases blog Michael Misch takes us through a case of accidental hypothermia and cardiac arrest, reviewing the controversies in management as well as the guidelines for rewarming, the role of ECMO and the alterations to ACLS cardiac arrest medications, CPR and defibrillations.
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. Further information is not available.
Case: You are the medical director of an EMS system in a large city deciding on whether to respond to all out of hospital cardiac arrests (OHCA) with ACLS capabilities, or if resources should be directed to those candidates for extracorporeal CPR. Bystander high-quality CPR can buy you some time until defibrillation.
After reviewing over 12 million EMS incidents that took place in 2023 , the 2024 ESO EMS Index highlights two critical areas that demand attention: Early CPR and Opioid Use Disorder (OUD). The importance of early CPR The earlier CPR is performed, the better the outcome. Gender disparities were also found. Want to learn more?
A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Background: Airway management strategies for out of hospital cardiac arrest (OHCA) have been hotly debated since the dawn of CPR.
Bystander CPR is initiated prior to EMS arrival. One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. We now know that an emphasis on the basics (high quality chest compressions and defibrillation) are the most important aspects of resuscitation.
You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. Case: A 51-year-old man experiences a cardiac arrest on the street. He is unsuccessfully shocked.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
A recent case has highlighted the extraordinary potential of a novel intervention: triple-sequential defibrillation. The Case Unfolds Despite 82 minutes of high-quality CPR and Advanced Cardiovascular Life Support (ACLS) management, standard and dual-sequential defibrillation failed to restore the patient’s heartbeat.
Your team begins high quality cardiopulmonary resuscitation (CPR). Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base. Sodium bicarbonate has historically been used during CPR with the goal of alkalizing blood pH and treating metabolic acidosis.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). ECMO Flow was achieved after approximately 1 hour of high quality CPR. After good ECMO flow was established, she was successfully defibrillated. The K was normal. Troponin I rose to 44.1
They started CPR. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. This patient was witnessed by bystanders to collapse. After 1 mg of epinephrine they achieved ROSC.
Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation? 2,3 Multiple published studies have addressed treatment of ventricular fibrillation with defibrillation and medications such as amiodarone and lidocaine.
CPR is currently in progress with a single shock having been delivered. This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), and epinephrine ( SGEM#238 ).
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Head Up (HUP) CPR may be the next critical improvement. Head Up (HUP) CPR may be the next critical improvement. Resuscitation 2022; 179: 9-17.
There was no bystander CPR. He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. An elderly man collapsed.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). She has a history of hypertension and non-insulin dependent diabetes mellitus.
With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. Consider administering epinephrine after defibrillation in those with shockable rhythms. For patients with OHCA, use of steroids during CPR is of uncertain benefit.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
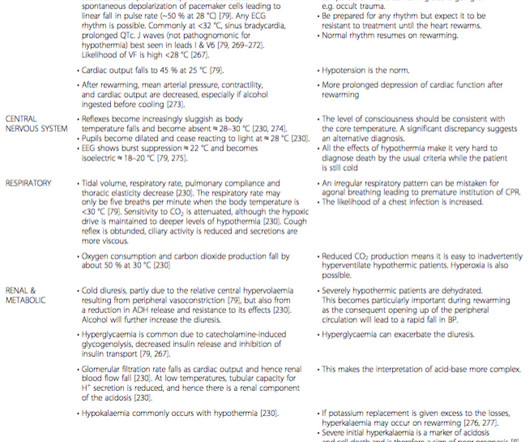
age, co-morbidities, trauma) (3) speed of cooling (4) environment (air, water, snow) (5) CA features (body temperature; whether hypoxia preceded arrest; delay before instituting CPR, and CPR quality) (6) rescue considerations (e.g. International guidance differ on drug administration. Many arrhythmias (e.g.
The elderly woman had gone into cardiac arrest just minutes before you arrived, but immediate CPR and rapid defibrillation were rewarded with a weak return of pulses. The call is going smoothly. Your IV is flowing and the patient is intubated.
This is a potentially fatal mistake because for VF, the one intervention besides CPR that is proven to increase survival to hospital discharge is defibrillation (but not for PEA). AHA CPR Guideline 2015: In addition to high-quality CPR,
I recerted CPR, ACLS (Advanced Cardiac Life Support) and PALS (Pediatric Advanced Life Support) late in December. When you are doing CPR and running cardiac arrests on a regular basis, it seems unnecessary to sit through a 2 hour class on CPR and 4 hour classes on ACLS and PALS. The certs are good for two years. mg via syringe.*
The conversation covers topics such as compression-only CPR, the controversy surrounding head-up CPR, the use of band and piston-driven devices, and the potential of extracorporeal cardiopulmonary resuscitation (eCPR). The importance of good dispatch and patient selection is emphasized as key factors in improving outcomes.
defibrillator is a lifesaving piece of medical equipment which delivers an electrical shock to a cardiac arrest victim. Currently less than 10% of these people experiencing cardiac arrests in the community surviveAEDs are used in addition to CPR to save the lives of those suffering cardiac arrest. What is an AED and how to use one.A
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. After resuming CPR and administering an additional 400 mcg IV NTG, the patient achieved return of spontaneous circulation with sinus tachycardia. Click to enlarge.)
It was witnessed, and CPR was performed by trained individuals. She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. References : 1.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. His family has been performing bystander, and report that he suddenly collapsed just a few minutes ago.
covering prehospital medical providers — recognizes three levels of EMTs/paramedics: EMT: EMTs provide non-invasive life-support services, such as cardiopulmonary resuscitation (CPR), administering oxygen, performing automated external defibrillation, basic and advanced airway management, and administering authorized medications.
After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. This rhythm reportedly produced no palpable pulse, and CPR was continued. 30 seconds later, however, the patient began spontaneously moving and CPR was discontinued.
Similarly, funds can help purchase new defibrillators for paramedics, ensuring they have access to reliable equipment during critical life-saving moments. These programs might include open houses at fire stations, community CPR classes, or public safety demonstrations.
If the victim is unresponsive, CPR is initiated immediately. We use portable electrocardiogram (ECG) machines to monitor heart rhythms and are equipped to administer life-saving interventions like defibrillation or medication administration to stabilize the heart rhythm.
CPR was started immediately. She was never defibrillated. As was seen in this case — defibrillation and/or overdrive pacing may be needed. A 60-something woman presented after a witnessed cardiac arrest. EMS arrived and found her in a wide complex PEA rhythm.
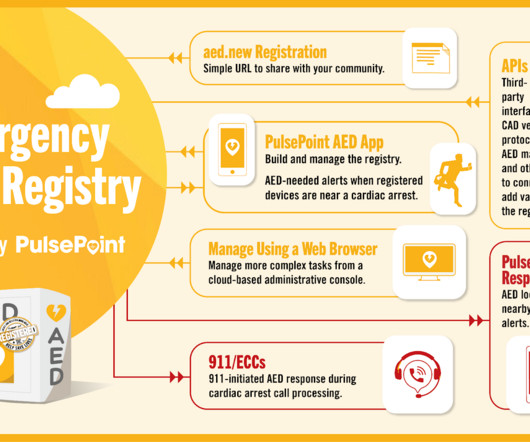
October is Sudden Cardiac Arrest Awareness month, so High Performance EMS and PulsePoint are encouraging everyone to locate and register Automated External Defibrillators (AEDs). It’s relatively recent that providing CPR instructions to callers (t-CPR) was considered best practice.
12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC. In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts.
We could not resuscitate her, but we did have excellent perfusion with LUCAS CPR, such that pulse oximetry had excellent waveform and 100% saturations, end tidal CO2 was 35, and cerebral perfusion monitoring was near normal throughout the attempted resuscitation. How would you treat?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content