This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this call, paramedics arrived on scene to find a patient apneic and pulseless with CPR in progress by first responders (AED had an unknown unshockable rhythm). Patient had an unwitnessed cardiac arrest without bystander CPR performed. Pacing was continued in the ED, with identical settings. Several learning points here.
The paramedics begin CPR. CPR is performed with manual compressions as no mechanical CPR device is available. They are unable to feel a pulse and resume CPR. On ED arrival ROSC is achieved. Suddenly, the patient has a bowel movement and becomes pulseless / apneic. Intubation is attempted, but unsuccessful.
The post EM Quick Hits 23 – Clinical Probability Adjusted D-dimer, ARDS Part 2, Pharyngitis Mimics, Barotrauma, Vertigo, CPR Gender-Based Differences appeared first on Emergency Medicine Cases.
In this part 2 of our 2-part podcast series on Cardiac Arrest - The When, Why & How, we discuss some of the finer art of cardiac arrest care and answer questions such as: how should we best communicate to EMS, the ED team and the family of the patient to keep the team focused, garner the most important info and keep the flow of the code going?
He currently practices emergency medicine in New Mexico in the ED, in the field with EMS and with the UNM Lifeguard Air Emergency Services. On arrival, you find a 35-year-old male, pulseless and apneic with cardio-pulmonary resuscitation (CPR) in progress by a bystander. There is drug paraphernalia scattered around the room.
Yoo, MD (Assistant Professor/Core Faculty, San Antonio, TX) // Reviewed by Brit Long, MD (@long_brit) Case An 18-year-old man with a history of asthma and medication noncompliance presents to the emergency department (ED) with acute onset shortness of breath. He states that he recently moved to Texas from Colorado. Which one do you select?
After reviewing over 12 million EMS incidents that took place in 2023 , the 2024 ESO EMS Index highlights two critical areas that demand attention: Early CPR and Opioid Use Disorder (OUD). The importance of early CPR The earlier CPR is performed, the better the outcome. Gender disparities were also found.
When emergency department (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. This is because of the ease of finding anatomic landmarks and their location away from other procedures like defibrillation, CPR, and airway management. The classic location for IO placement is the tibial plateau.
I remember when I started practicing emergency medicine a decade and a half ago it seemed that any kid who came to our ED in cardiac arrest died. I know, depressing thought. But, over the past 15 years, survival to discharge from pediatric cardiac arrest has markedly improved, at least for in-hospital arrests.
Case: A 6-month-old boy presents to the emergency department (ED) with three days of worsening cough, cold symptoms, and fever. Your team begins high quality cardiopulmonary resuscitation (CPR). Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU). Pediatric Crit Care Med.
Case: You are working at the community emergency department (ED) when you receive a call from the local Emergency Medicine Service (EMS) team that they are bringing a 2-year-old boy who had a cardiac arrest at home. They started cardiopulmonary resuscitation (CPR) until EMS arrived.
75 year old man was brought to ED by ambulance in VF cardiac arrest , CPR in progress. His venous blood gases showed the following PH = 7.14 pCO2 = 53 mmHg
A 4 week old is brought to ED post cardiac arrest – the child was found in her cot not breathing. The parents performed CPR immediately and on arrival the child had ROSC. The child has been unwell …
A 4 week old is brought to ED post cardiac arrest – the child was found in her cot not breathing. The parents performed CPR immediately and on arrival the child had ROSC. The child has been unwell …
85 years old lady with history of COPD, brought to ED with low GCS after VF cardiac arrest and return of spontaneous circulation after 3 minutes of CPR and a single DC shock. Her VBG on arrival sho…
85 years old lady with history of COPD, brought to ED with low GCS after VF cardiac arrest followed by return of spontaneous circulation after 3 minutes of CPR and a single DC shock. Her VBG on arr…
A 7 year old boy is brought to ED with his mother with a 4 day history of abdominal pain and vomiting. O/E BP 90/50 HR 115 Sats 97% RA Temp 37 RR 30 CPR 4 seconds. He has no PMH. The child has sunk…
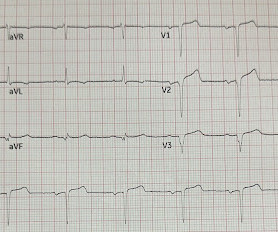
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? No Chest Pain, but somnolent.
Case: During a busy emergency department (ED) shift the paramedic phone rings. CPR is currently in progress with a single shock having been delivered. On the other end of the line is one of your local crews who have responded to a 54-year-old male with a witnessed cardiac arrest.
Missy is also now the director for Difficult Airway EMS course in Washington State Case: An EMS crew arrives to your emergency department (ED) with a 58-year-old female who suffered a witnessed ventricular fibrillation (VF) out-of-hospital cardiac arrest (OHCA). Background: We have covered OHCA multiple times on the SGEM.
Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model in post ROSC patients. Episode 98: Post ROSC Mental Model What’s the problem?
Authors: Rebecca Dupree, DO and Emerson Franke, MD FAEMS FAAEM Case The dreaded scenario: youre performing high quality CPR in the field, youve successfully intubated the patient, and suddenly you hear, I found their DNR form! These may result in an ED extubation or admission to the hospital for comfort care and terminal extubation.
Listen to the ED ECMO podcast on ECPR here Find us on Patreon here! Listen to the ED ECMO podcast on ECPR here Find us on Patreon here! No-flow time without CPR should be very brief (witnessed is best), but low-flow time (with CPR) can actually be very long and still have good outcomes with ECPR. Buy your merch here!
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. ED attendings Dr. Gerald Whelan and Dr. Shumary Chow supervising a full arrest in C booththe main trauma roomwith an ED tech administering CPR. Click to enlarge.)
CPR was ongoing, and their ETA was 10 minutes. We prepared the ED for the patient’s arrival. In Fall 2023, I was working an evening shift at a community hospital when we got a patch. A 3-year-old girl was being brought in by EMS with an out-of-hospital cardiac arrest. It’s Backkkk (Part 1) appeared first on EMOttawa Blog.
She was intubated at the scene and transported to your ED, with cardiopulmonary resuscitation (CPR) performed en route. Despite good quality CPR, there is no ROSC. Despite good quality CPR, there is no ROSC. Despite good quality CPR, there is no ROSC. Emergency Medical Services found her apneic and pulseless.
Even though sedation after endotracheal intubation (ETI) reduces the risk of self-extubation, uncontrolled pain, and awakening awareness, several small single-centre studies demonstrate low rates of sedative drug administration after ETI in the emergency department (ED). This is referred to as CPR I nduced C onsciousness ( CPRIC ).
CASP checklist for Clinical Prediction Rule (CPR) studies Is CPR clearly defined? A proportion of participants were missed because the ED provider refused enrollment or said “Other,” but this is not well described. I am hopeful it will also improve the flow in the ED.”
Duties include but are not limited to stocking, cleaning, transporting patients, performing EKGs, blood draws, and CPR. It's important to keep in mind that you are not functioning as an EMT when you're an ED Tech/Assistant.
Guest Skeptic: Dr. Neil Dasgupta is an emergency physician and ED intensivist from Long Island, NY, and currently an assistant clinical professor and Director of Emergency Critical Care […] The post SGEM#350: How Did I Get Epi Alone? Cardiopulmonary resuscitation (CPR) is in progress. JAMA Sept 2021.
There was no bystander CPR. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines.
They carry the same CPR card in their wallets as I do, they readily use the brains between their ears, so why are we made to perform futile efforts on a patient who didn’t want the help to begin with? A clinically primitive mindset; no heartbeat bad, CPR good, liability avoided. Does that mean a little more training or continuing ed?
They started CPR. The patient was brought to the ED and had this ECG recorded: What do you think? This patient was witnessed by bystanders to collapse. EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. sodium bicarbonate.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergency department (ED). His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. It is unclear how long he was down.
Case: A 59-year-old woman comes is brought into your emergency department (ED) by EMS in cardiac arrest. She had a witnessed arrest, and CPR was initiated by bystanders. The patient achieved return of spontaneous circulation (ROSC) on arrival to the ED.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. For clarity — I’ll again show the initial ECG done in the ED in Figure-1. She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support).
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. “Code,” “No Code,” “CPR,” “resuscitation,” etc. To opt in to the free subscriber list, click here. Stories of med mal lawsuits can save lives.
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC.
Bystander CPR. He went in and out of arrest until arrival at the ED. Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? A patient was found down approximately 30 minutes after taking methamphetamine. Medics found patient in PEA arrest.
This post will focus on the key parts of the guideline that affect ED evaluation and management. For patients with OHCA, use of steroids during CPR is of uncertain benefit. Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association 2023 Guideline Updates for 2023 were just published.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content