This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia.
Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model in post ROSC patients. Episode 98: Post ROSC Mental Model What’s the problem?
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
They started CPR. The patient was brought to the ED and had this ECG recorded: What do you think? Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. sodium bicarbonate. sodium bicarbonate.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). He reports feeling nauseated with emesis. The Queen was not used in real time. Even the Queen can be wrong.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. I believe the latter (type II STEMI) is most likely. Troponin I rose to 44.1
This post will focus on the key parts of the guideline that affect ED evaluation and management. For patients with OHCA, use of steroids during CPR is of uncertain benefit. Editorial Comment : Yes to PCI after arrest with STEMI on ECG. Major Updates Avoid routine use of calcium in patients with cardiac arrest. COR 2b, LOE B-R.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
One of these areas is assessing patients with ED-diagnosed strokes. Currently, conventional EMS education tends to center symptoms of a STEMI or NSTEMI for males as “typical” and females as “atypical.” One area we found in need of improvement is bystander CPR.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). He appeared to be in shock.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
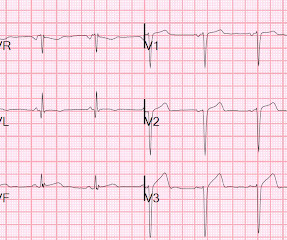
Here is his ECG on presentation to the ED, approximately 45 minutes after onset of pain, but with pain improving since onset: What is your interpretation? The initial ECG was interpreted as "normal" by the computer ( Algorithm: Marquette GE / 12SL ) and "no acute ischemic changes" by the ED physician.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Which was the culprit lesion?
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery? The pattern seen may, or may not, be unique to left main occlusion.
About an hour later, he was then found on the floor in cardiac arrest in the ED. He underwent CPR and then was shocked out of VF. The history in today's case — was that of a man in his 70s who presented to the ED for 2 hours of chest pain , that was still present on arrival in the ED. But we should not be surprised.
Her prehospital ECG was identical to her first ED ECG, and the cath lab was activated: There is massive ST elevation (greater than 15 mm) in V2 and V3, with ST elevation in I and aVL and reciprocal ST depression in II, III, aVF. Peterson ED, Hathaway WR, Zabel KM, et al. Hathaway WR, Peterson ED, Wagner GS, et al.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
I would rather use a PCAC score to decide on transfer than arrest characteristic (time of CPR, initial rhythm, etc) because we know that all of that data is prone to bias as well. We hope that PCAC would be similar, but I’m not sure we have enough data to be sure. Right now, we do not use PCAC in our decisions to transfer or not, by the way.
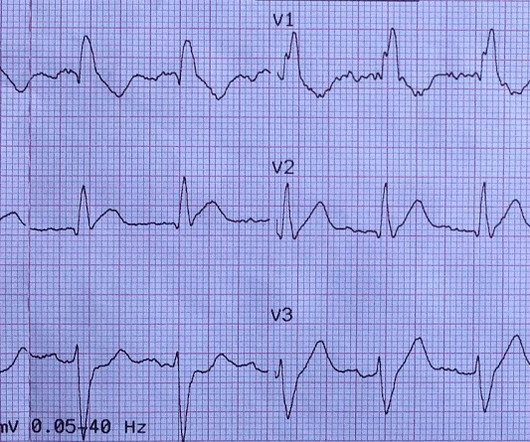
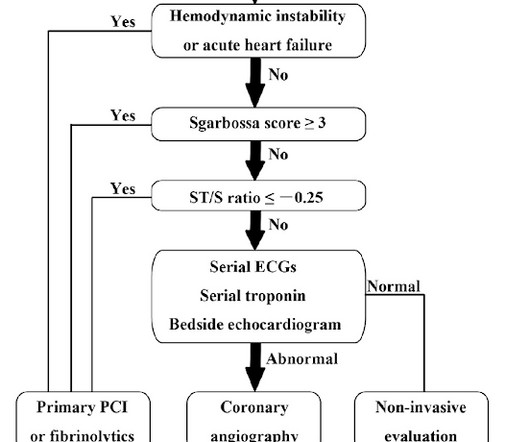
Were not obviously hitting Sgarbossas critera, so I wouldnt activate a STEMI alert, but it sure doesnt look good. The patient has no pulse so you start CPR. From the EDs point of view, we really only use the first 3. Remember pacemakers rely on muscle to muscle spread of electrical activity, so we expect a wide QRS.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content