This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
When emergencydepartment (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. This is because of the ease of finding anatomic landmarks and their location away from other procedures like defibrillation, CPR, and airway management. The classic location for IO placement is the tibial plateau.
You’re in the paediatric emergencydepartment, typing some notes for the child you’ve just discharged. They’re getting CPR. Promoting hot debriefing in an emergencydepartment. Scand J Trauma Resusc Emerg Med. Emergency Medicine Residents Experience Acute Stress While Working in the EmergencyDepartment.
JAMA 2018 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a physician assistant practicing in emergency medicine in the Seattle area and an adjunct faculty member with the Tacoma Community College paramedic program. It required multiple attempts which caused several prolonged interruptions in CPR.
Bystander CPR is being performed. The paramedics performed high-quality CPR and follow their ACLS protocol. CPR is continued while a supraglottic airway is placed successfully. The patient is transported to the emergencydepartment with vital signs absent (VSA). The monitor is hooked up.
Case: A 6-month-old boy presents to the emergencydepartment (ED) with three days of worsening cough, cold symptoms, and fever. Your team begins high quality cardiopulmonary resuscitation (CPR). Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base.
Authors: Rebecca Dupree, DO and Emerson Franke, MD FAEMS FAAEM Case The dreaded scenario: youre performing high quality CPR in the field, youve successfully intubated the patient, and suddenly you hear, I found their DNR form! Death and End-of-Life Care in EmergencyDepartments in the US. just as youve gotten ROSC. Statista.
She is part of the Don’t Forget the Bubbles team and faculty at Queen Mary University in London where she teaches part of the Paediatric Emergency Medicine MSc. They started cardiopulmonary resuscitation (CPR) until EMS arrived. He had been having some upper respiratory symptoms in the previous days.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services at Tacoma Community College. Case: During a busy emergencydepartment (ED) shift the paramedic phone rings.
Missy is also now the director for Difficult Airway EMS course in Washington State Case: An EMS crew arrives to your emergencydepartment (ED) with a 58-year-old female who suffered a witnessed ventricular fibrillation (VF) out-of-hospital cardiac arrest (OHCA). Background: We have covered OHCA multiple times on the SGEM.
You are the Paediatric doctor on call and receive a call for an incoming patient to the emergencydepartment. Tragically, several attempts at resuscitation upon arrival at the emergencydepartment were unsuccessful. This is referred to as CPR I nduced C onsciousness ( CPRIC ). Ann Emerg Med. His name is Ben.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. She has a history of hypertension and non-insulin dependent diabetes mellitus.
He is currently deployed, practicing emergency medicine in an undisclosed location. Case: You are working a regular shift in the emergencydepartment when you hear a code blue called. SGEM#64 : Classic EM Papers (OPALS Study) * SGEM#136 : CPR – Man or Machine?
Neil Dasgupta is an emergency physician and ED intensivist from Long Island, NY, and currently an assistant clinical professor and Director of Emergency Critical Care at Nassau University Medical Center. Case: A code blue is called for a 71-year-old male in-patient that is boarding in the emergencydepartment (ED).
PECARN prediction rule for cervical spine imaging of children presenting to the emergencydepartment with blunt trauma: a multicentre prospective observational study. CASP checklist for Clinical Prediction Rule (CPR) studies Is CPR clearly defined? Lancet Child Adolesc Health. 2024 Jun 3:S2352-4642(24)00104-4.
The photos that Dr. Clarke took from 19781980 provide a glimpse into working in an emergencydepartment in the years the specialty was being established. ED attendings Dr. Gerald Whelan and Dr. Shumary Chow supervising a full arrest in C booththe main trauma roomwith an ED tech administering CPR. Click to enlarge.)
Yoo, MD (Assistant Professor/Core Faculty, San Antonio, TX) // Reviewed by Brit Long, MD (@long_brit) Case An 18-year-old man with a history of asthma and medication noncompliance presents to the emergencydepartment (ED) with acute onset shortness of breath. He states that he recently moved to Texas from Colorado.
Laura Melville ( @lmelville535 ) is an emergency physician in Brooklyn, New York, is a part of the New York ACEP Research Committee, ALL NYC EM, and is the NYP-Brooklyn Methodist Resident Research Director. Case: A 59-year-old woman comes is brought into your emergencydepartment (ED) by EMS in cardiac arrest.
After resuming CPR and administering an additional 400 mcg IV NTG, the patient achieved return of spontaneous circulation with sinus tachycardia. This case report documents the first known instance of using NTG during an emergencydepartment resuscitation to treat a patient in cardiac arrest due to severe coronary artery vasospasm.
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). ECMO Flow was achieved after approximately 1 hour of high quality CPR. An elderly woman had sudden ventricular fibrillation.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergencydepartment (ED). You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Am J Emerg Med. 1996;40(3):483-485. Accidental hypothermia.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Staff interrupt you while you’re in Room 3 with a patient you’ve placed on BiPAP, “We have an incoming patient with CPR in progress in five minutes,” the nurse says before adding, “Room 4’s family really wants to talk with you again.” Dr. Koo is an emergency physician and attending at MedStar Washington Hospital Center in Washington, and St.
Every year, countless young lives are impacted by the split-second decisions made in emergencydepartments across the United States. Only 14% of emergencydepartments are adequately ready to manage pediatric emergencies, a statistic that speaks volumes about the silent risks our children face. Florida Senate.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
Introduction: Civility Matters Healthcare environments, particularly emergencydepartments, are characterised by high levels of Volatility, Uncertainty, Complexity, and Ambiguity ( VUCA ). A third RCT demonstrated that even brief low-level incivility could increase the risk of major error during CPR by up to 66%.
Recognizing the Difference Between EMTs, AEMTs, and Paramedics The National Registry of Emergency Medical Technicians (NREMT) — that’s the leading certification agency in the U.S. Some EMT courses require CPR as a prerequisite, while others, including ours, include CPR training and certification.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. The take home message: “Irrespective of presenting rhythm, in patients with cardiac arrest, there is no conclusive evidence that administration of calcium during cardiopulmonary resuscitation (CPR) improves survival.” Wongtanasarasin, W.,
Optimally, bystander CPR, including the administration of rescue breaths, should be initiated prior to arrival of emergency medical services. 3 Once the patient arrives in your emergencydepartment, a rapid review of the patient’s status and results of resuscitative efforts should be performed. Am J Emerg Med.
But since the mid 80s, we have realized that EMS is the clinical practice of emergency medicine outside of the emergencydepartment. Emergency physicians who are not EMS specialized can turn to a number of resources for assistance. But there weren’t the physician resources to support that need,” he said.
When emergency medical services (EMS) arrived, she was in asystole with an empty, recently full, bottle of benzonatate 100 mg capsules. She received cardiopulmonary resuscitation (CPR) and standard advanced cardiovascular life support (ACLS). Upon ED arrival, she had a heart rate (HR) of 160 and blood pressure (BP) of 80s/40s.
How to stop bleeding, perform CPR, and assist breathing. Many fire departments require that all of their firefighters also be EMTs. They respond to medical emergencies and provide treatment on scene to assist the ambulance crews. First Aid and to how to respond to a cardiac arrest.
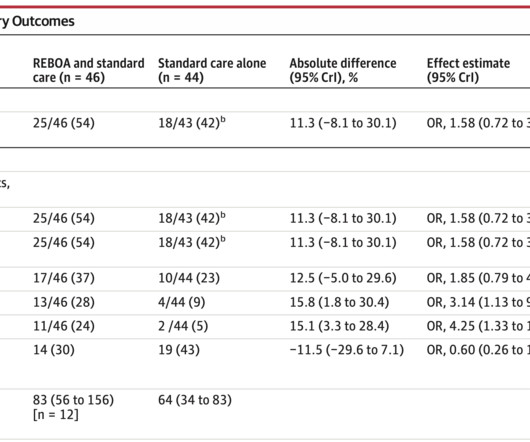
EmergencyDepartment Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial [published online ahead of print, 2023 Oct 12]. The enrolled population was severely injured, with a median ISS of 41, and 23% received CPR.
These can include feeling compelled to attempt resuscitation despite the team feeling it is futile or not consistent with the patient’s wishes, families demanding CPR despite the presence of a DNR, incompletely filled out DNR forms, and more. had performed CPR on a hospice patient, and 17.9% Prehosp Emerg Care. PMID: 35490992.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Interventions during the acute phase of treatment post return of spontaneous circulation (ROSC) are therefore critical.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. A middle-age woman with h/o hypertension was found down by her husband. With ventilations and epinephrine, she regained a pulse.
Question While performing one-person CPR on a patient, you should use a ratio for compressions to ventilation for the adult patient and a __ ratio for a child patient. Apply an AED Begin CPR Correct Incorrect Question 2 of 10 2. Provide two minutes of CPR prior to attaching the AED. Apply a nonrebreather at 15 lpm.
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergencydepartment, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute Myocardial Infarction in the EmergencyDepartment Case 1.
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury.
This single-centre academic urban institution in the United States (US) undertook a 10-year retrospective observational study of paediatric intubation and bougie use in their emergencydepartment (ED). Reviewed by: Roberto Segura and Mel Ranaweera Article 3: Does hand position affect CPR quality in young children? Resuscitation.
Data was collected at 2 emergencydepartments in America and included assessment by both clinicians and patients for a total of 31 patients. The device was assessed by the clinicians (emergency medicine doctors) using it on ease of use, speed of use and the appearance of the closed wound. Why does it matter?
A notable achievement was ESEM’s co-organization of the International Federation of Emergency Medicine Trauma Update Symposium in 2015. These initiatives aim to equip physicians with an evidence-based approach and effective management strategies for common emergency-department scenarios.
A 67-year-old man presents to the emergencydepartment (ED) in cardiac arrest. 1 Overall, survival is poor following cardiac arrest, and is affected by factors including age, comorbidities, witnessed arrest, early CPR, early defibrillation, and return of spontaneous circulation (ROSC).
In fact, 4000 paramedics in total were not only trained in the study protocol but also given a rigorous evaluation of their ability to perform CPR. On the topic of EMS and similar to the pilot study, there was an incredibly high amount of bystander CPR performed. Thus limiting the external validity of this paper’s findings.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content