This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this month's EM Quick Hits podcast: Anand Swaminathan on lateral canthotomy, Emily Austin on pediatric cannabis poisoning, Reuben Strayer on an approach to hyperthermia, Brit Long on diagnosis and management of malignant otitis externa, Jesse McLaren on ECG diagnosis of occlusion MI in patients with BBB and Peter Brindley on prone CPR.
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
They started CPR. EMS arrived and found him in Ventricular Fibrillation (VF). Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC.
There are steps to take to work towards closing this gap, such as not prioritizing a set list of symptoms as “normal EKG” and recognizing atypical presentations across different patient populations. EMS services can proactively work to improve how they communicate within their communities.
This is an extremely important topic especially for EMS systems that are implementing High Performance CPR , because it is very predictable that you are going to see a lot more patients with return of pulses in the field, and if you don’t have a plan, lots of things can go wrong before arriving at the hospital.
Appropriate air medical services utilization and recommendations for integration of air medical services resources into the EMS system of care: a joint position statement and resource document of NAEMSP, ACEP, and AMPA. Air medical transport has been utilized in multiple hospital based programs including trauma, STEMI, and stroke.
He received aspirin en route via EMS, and no EMS ECGs are available. This rhythm reportedly produced no palpable pulse, and CPR was continued. 30 seconds later, however, the patient began spontaneously moving and CPR was discontinued. A repeat ECG was done: Obvious anterolateral wall STEMI.
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. In these cases, thrombolysis is recommended to improve morbidity and mortality. Primary PCI: 95.7%
Did they get bystander CPR? PMID: 37634145 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The ECLS-SHOCK Trial: ECPR in Infarct-Related Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog. Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Control: 49.0% RR 0.98; 95% CI 0.80
EMS recorded the following ECG: What do you see? Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. A male in late middle age with a history of RCA stent 8 years prior complained of chest pain.
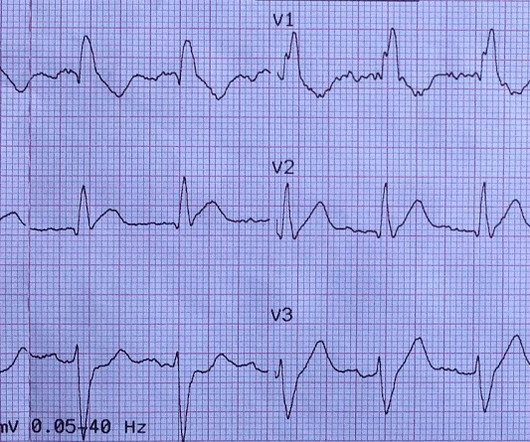
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
CPR was initiated immediately. The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
I would rather use a PCAC score to decide on transfer than arrest characteristic (time of CPR, initial rhythm, etc) because we know that all of that data is prone to bias as well. The post External Validation of Pittsburgh Cardiac Arrest Category (PCAC) Illness Severity Score appeared first on REBEL EM - Emergency Medicine Blog.
Authors: Lloyd Tannenbaum, MD (EM Attending Physician, Geisinger Wyoming Valley, PA) // Reviewer: Brit Long, MD (@long_brit) Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. The patient has no pulse so you start CPR. Please check it out. You yell at him, Are you ok?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content