This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this month's EM Quick Hits podcast: Anand Swaminathan on lateral canthotomy, Emily Austin on pediatric cannabis poisoning, Reuben Strayer on an approach to hyperthermia, Brit Long on diagnosis and management of malignant otitis externa, Jesse McLaren on ECG diagnosis of occlusion MI in patients with BBB and Peter Brindley on prone CPR.
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.
Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model in post ROSC patients. Episode 98: Post ROSC Mental Model What’s the problem?
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. There is evidence that taking those patients with ROSC and EKG showing STEMI directly for angiography +/- angioplasty is associated with positive patient-oriented outcomes.
The nurses started CPR immediately and place pads before you even arrived. A post-arrest ECG doesn’t show any signs of STEMI. A 50-year-old man who was admitted to the hospital with a non-ST elevated myocardial infarction (NSTEMI) overnight was found unconscious and without a pulse. The patient is still unconscious.
They started CPR. Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. I believe the latter (type II STEMI) is most likely. Troponin I rose to 44.1
For patients with OHCA, use of steroids during CPR is of uncertain benefit. Extracorporeal CPR Use of ECPR for patients with cardiac arrest refractory to standard ACLS is reasonable in select patients when provided within an appropriately trained and equipped system of care. COR 2b, LOE B-R. COR 2b, LOE C-LD.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Working towards better detection Another area ESO has identified as an opportunity to improve is how EMS services detect a possible STEMI or NSTEMI with a 12-lead EKG. Currently, conventional EMS education tends to center symptoms of a STEMI or NSTEMI for males as “typical” and females as “atypical.”
This is an extremely important topic especially for EMS systems that are implementing High Performance CPR , because it is very predictable that you are going to see a lot more patients with return of pulses in the field, and if you don’t have a plan, lots of things can go wrong before arriving at the hospital.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The following 12-lead ECG was recorded at 11 minutes after ROSC. see below).
This rhythm reportedly produced no palpable pulse, and CPR was continued. 30 seconds later, however, the patient began spontaneously moving and CPR was discontinued. A repeat ECG was done: Obvious anterolateral wall STEMI. Beats 4, 6, and 7 are narrow, as the rhythm is trying to resume from above the ventricles.
Air medical transport has been utilized in multiple hospital based programs including trauma, STEMI, and stroke. Cardiac arrest has been proven difficult in flight, but research is still needed with mechanical CPR machines. They have also been utilized with high risk OB, specialized patients with IABP, ECMO, Impella’s etc.
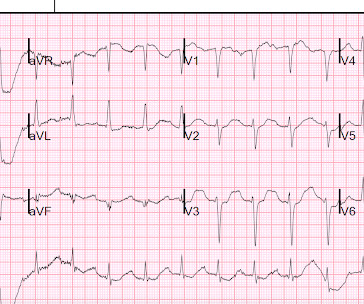
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology.
He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. The physician recorded this ECG, interpreted it as normal, and sent the patient home on an antacid. See explanation below. The patient went home and, in front of his wife, he collapsed. I do not have the post-resuscitation ECG.
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. When the ECG shows the effects of hypokalemia, it is particularly dangerous. There is particularly little on how to treat when the K is less than 2.0,
Might be a good idea to revisit this) You likely practice CPR, cannulation, airway insertion and all the fun stuff, but I guarantee that you will spend more time talking on the radio than doing those things. It therefore makes sense to practice communication as well. Learn it, use it.
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
He underwent CPR and then was shocked out of VF. Both hyperacute T waves and posterior OMI are now formally endorsed as "STEMI equivalents" by the ACC. == MY Comment, by K EN G RAUER, MD ( 11/23 /2022 ): == Cases in which initial ECG findings are subtle before undergoing dramatic change, — are always impressive.
to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 I could find very little literature on the treatment of severe life-threatening hypokalemia. If 10 mEq is given very rapidly, leaving no time for intracellular shift, then it will raise serum K by about 3.3 If the patient is at 1.8, that will raise it to 5.1
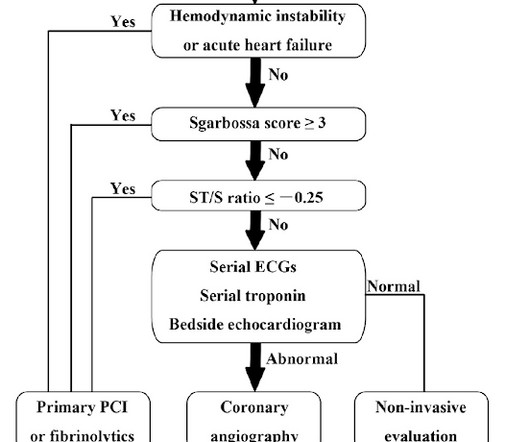
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. In these cases, thrombolysis is recommended to improve morbidity and mortality. Primary PCI: 95.7%
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). He reports feeling nauseated with emesis. The Queen was not used in real time. Even the Queen can be wrong.
Did they get bystander CPR? Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Majority of patients had PCI performed (96.6%) Impella CP was most common mechanical circulatory support in patients without ECLS (85.7%) Death From Any Cause at 30d ECLS: 47.8% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 Control: 9.6% Control 3.8%
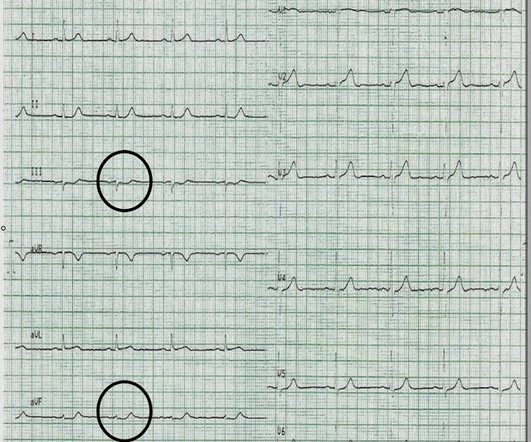
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. He was intubated and then went pulseless.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Kurkciyan et al.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." It does take some time for thrombus to form, but the EKG and the troponin profile show that this was NOT a late presentation STEMI. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0
CPR was initiated immediately. Decision was made to push tPA after approximately 25 minutes of CPR, and after approximately 25 minutes after tPA was given, O2 saturation increased to 97%, and the patient was no longer cyanotic, converted to normal sinus rhythm with anterior lateral T wave inversions with ST depressions."
I would rather use a PCAC score to decide on transfer than arrest characteristic (time of CPR, initial rhythm, etc) because we know that all of that data is prone to bias as well. We hope that PCAC would be similar, but I’m not sure we have enough data to be sure. Right now, we do not use PCAC in our decisions to transfer or not, by the way.
Were not obviously hitting Sgarbossas critera, so I wouldnt activate a STEMI alert, but it sure doesnt look good. The patient has no pulse so you start CPR. Narrow QRS complexes Morphology: no ST elevation concerning for STEMI Final read: I had to do a double take on this one. The QTc also looks maybe a little prolonged.
Stoic stalwarts are becoming more likely to call when they suffer a STEMI, rather than putting it off until it’s too late. Bystanders are growing to relish the thought of CPR and saving a life now that the concept is less foreign and frightening.
Angiography was technically challenging as the patient was receiving CPR, but the cardiologist suspected acute stent thrombosis and initiated cangrelor, although no repeat angiography was able to be obtained. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content