This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Hosts: Joe Offenbacher, MD Audrey Bree Tse, MD [link] Download Leave a Comment Tags: Anticoagulation , CriticalCare , Resuscitation Show Notes Coagulation Cascade: Algorithm for Anticoagulated Bleeding Patient in the ED: Indications for Anticoagulation Reversal: References: Baugh CW, Levine M, Cornutt D, et al.
Takeaway lessons * In an ideal world, penetrating abdominal trauma in an unstable patient would proceed directly to the OR with no delay by the ED. Not too much role for TEG in the initial ED presentation. Continue to use a balanced ratio unless you can use TEG to guide FFP and platelets.* FFP is delayed or unavailable; 2.
A 37-year-old G5P4 at 33 weeks presents to the ED after being brought in by ambulance. Treatment is supportive with respiratory therapy, criticalcare, inotropic therapy, and cardiac life support. We’ll keep it short, while you keep that EM brain sharp. She had a precipitous delivery while the ambulance was pulling in.
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the usual filters of ED, medical team to the ward.
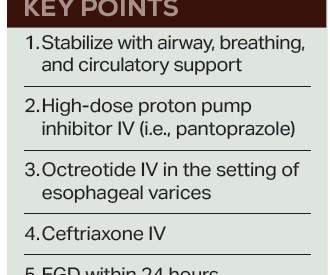
Fresh frozen plasma, or FFP, should only be given to cirrhotic patients as part of the massive transfusion protocol in cases of profound hypotension, as “patients with cirrhosis rarely have true enzymatic hypocoagulability, and FFP may worsen bleeding due to over-resuscitation and dilution of coagulation factors.”
Airway: Key decision: base decision for intubation on clinical course, efficacy of airway clearance (coughing, mental status), ED/institutional resources, respiratory status (respiratory failure). Warfarin: vitamin K 10 mg IV and PCC or FFP. Fibrinogen level < 150 mg/dL: cryoprecipitate or fibrinogen concentrate (not FFP).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content