This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
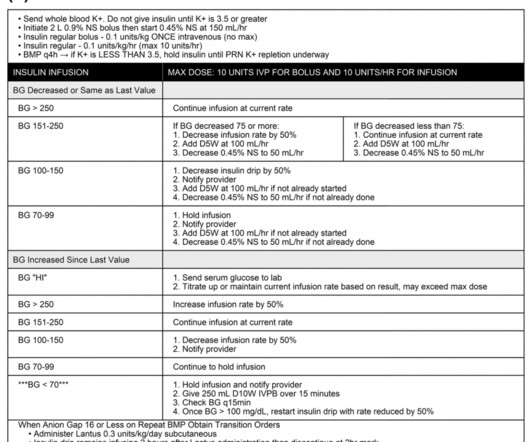
Case: A 28-year-old male with a history of type-1 diabetes mellitus presents to the emergencydepartment (ED) with increase in thirst and light headedness. The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip.
Fever in the EmergencyDepartment Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. CriticalCare Medicine 2017. Guest Skeptic: Jesse Spurr works as a Nurse Educator in the EmergencyDepartment at Redcliffe Hospital in Australia. CriticalCare Medicine 2017.
The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. It was found that patients exposed to deep sedation in the ED had an independent higher incidence of continued deep sedation on ICU day one ( Fuller, 2019 ).
Precedex (dexmedetomidine) is an alpha-2 adrenergic agonist increasingly used in criticalcare environments for sedation and anxiolysis. Historically, it has been used more frequently in the ICU than in EmergencyDepartments, likely due to provider comfort. […] The post Is there a Precedence for Precedex in the ED?
set out to explore in the Kids THRIVE study investigating whether NHF apnoeic oxygenation could improve intubation outcomes in critically unwell children needing emergency airway management. A total of eleven intensive care units (ten PICUs and one non-maternity NICU) and four emergencydepartments (EDs) took part in the study.
The Effect of Vitamin C on Clinical Outcome in Critically Ill Patients: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. CriticalCare Medicine. Guest Skeptics: Dr. Erin Willard is a PGY-3 Emergency Medicine Resident, Department of Emergency Medicine, University of Arkansas for Medical Sciences.
ClinicalTrials.gov: NCT02517489 7 Clinical Question: In adult patients with severe community-acquired pneumonia admitted to the ICU, does early hydrocortisone treatment, compared to standard therapy, reduce mortality at 28 days? Patients enrolled from 31 Intensive Care Units in France. ICU-acquired infections were observed in: 9.8%
Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Pediatric Crit Care Med. 2022 Date: February 15, 2023 Guest Skeptic: Dr. Carlie Myers is Pediatric CriticalCare Attending at Cincinnati Children’s Hospital Medical Center.
A heavy alcohol drinker, who is well known to your EmergencyDepartment, presents with altered mental status, except that he looks different this time. In our emergencydepartment, the RTs do not spend a lot of time going around measuring cuff pressures and usually save that until the patient reaches the ICU.
Anireddy Reddy is a pediatric intensive care attending physician in the Department of Anesthesiology and CriticalCare Medicine at Children’s Hospital of Philadelphia. Dr. Anireddy Reddy Case: A 3-year-old girl presents to the emergencydepartment (ED) with fever and respiratory distress.
2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Over the past few years, there has been an increase in emergencydepartment (ED) volumes and lengths of stay. J Crit Care. J Crit Care. Paper: Owyang CG, et al.
Intensive Care Med 2021 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a professor of Emergency Medical Services at Tacoma Community College’s paramedic program. Trial: Prospective, randomized, parallel-assignment, open-label, single-center trial ( NCT02643381 )
The Case A 24-year-old man with no past medical or surgical history presented to the emergencydepartment with 5 days of progressively worsening bilateral leg cramping, paresthesias, and multiple falls. The Internet Book of CriticalCare. Acute and emergencycare for thyrotoxicosis and thyroid storm.
Case: A 59-year-old woman presents to the emergencydepartment (ED) with fever, tachycardia, and hypotension. She is admitted to the intensive care unit (ICU) for septic shock. The ICU team is considering using Vitamin C therapy for this patient. The ICU team is considering using Vitamin C therapy for this patient.
Complications of Gluteal AFT The pale, prone patient with multiple surgical drains and a constrictive faja has become a common site in the Jackson Memorial Hospital EmergencyDepartment. Nearly half of all post-AFT patients presenting to our emergencydepartments required admission and six percent required ICU admission.
In most EmergencyDepartments, staff are allotted little of that scarce resource, time, to begin processing what has just occurred. The Pause Jonathon Bartels worked as an Emergency Nurse in America in 2009. After the death of a young person in the EmergencyDepartment, he initiated ‘ The Pause.’ 23 (2), pp.
A few rapid-fire cases from the emergencydepartment, with Dr. Seth Trueger (@mdaware), emergency physician at Northwestern University and digital media editor for JAMA Network Open. Continue reading "Episode 19: Emergency medicine with Seth Trueger" A few rapid-fire cases from the emergencydepartment, with Dr. .
Emergencydepartments (EDs) provide the essential service of evaluating patients with unscheduled, acute, undifferentiated, and decompensated conditions. Dr. Kluesner is an emergency physician in Iowa City, Iowa, at UnityPoint Health-Iowa Methodist Medical Center. Criticalcare medicine 40.8 PloS one 13.8
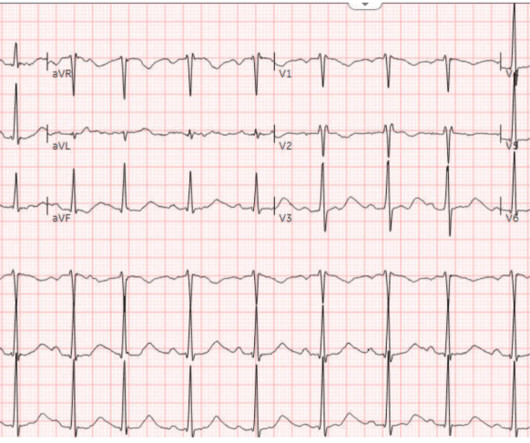
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the EmergencyDepartment (ED). 2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Am J Emerg Med. 2022 Sep 7.
If pre-made syringes are not financially feasible then the creation of these medications should be done by a dedicated emergencydepartment pharmacist. Clinical Bottom Line: Acute hypotension must be treated emergently in order to decrease morbidity and mortality. Intensive Care Med. Am J Emerg Med. J Med Toxicol.
The Importance of Civility in CriticalCare Resuscitation A 3-year-old patient with diabetic ketoacidosis arrives at your ED. The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. Conclusion Criticalcare resuscitation is stressful. How do you manage this situation?
Intravenous insulin infusions typically require treatment in highly monitored settings, such as an intensive care unit (ICU) or step-down unit for safety and due to the frequency and intensity of monitoring. ICU and step-down beds are a limited resource and generate higher hospital charges.
Alternatively, the Neurocritical Care Society defines it as a seizure with five minutes or more of continuous clinical or EEG seizure activity, or recurrent seizure activity without recovery between seizures. 1 History and physical examination have been the cornerstone of seizure diagnosis in the emergencydepartment (ED).
Ketamine vs etomidate in ICU intubation ? Etomidate versus ketamine for emergency endotracheal intubation: a randomized clinical trial. Preventing radial arterial catheter failure in criticalcare – Factoring updated clinical strategies and techniques. Anaesth Crit Care Pain Med. Emerg Med J.
1] Graduates of the combined degree may choose to work solely in either field, enter a subspecialty, pursue additional fellowship experience in criticalcare, or engage in research.[2] This path involves seventy-two months split between emergency medicine and internal medicine with additional experience in the criticalcare setting.[3]
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/criticalcare pod of your emergencydepartment (ED). You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Am J Emerg Med. 1996;40(3):483-485.
Management must be multidisciplinary involving anaesthetics, paediatric retrieval service/paediatric intensive care, ENT and oncology teams (as well as the cardiothoracic surgery team – not always available). Five-year-old Ginny presents to the EmergencyDepartment with a syncopal episode. A CXR demonstrates a mediastinal mass.
Background: Standard emergencydepartment management of acute pancreatitis has focused on aggressive hydration, analgesia and investigation for an underlying reversible cause (eg gallstones). Recent evidence has challenged the routine use of aggressive hydration as unnecessary. cc/kg/hour.
However, the decade since the original Hypothermia after Cardiac Arrest trial had seen significant advances in pre-hospital, emergencydepartment, and criticalcare that may have contributed to these outcomes. These results suggest that targeting a lower temperature of 33ºC confers no additional benefit to targeting 36ºC.
4 In an emergencydepartment (ED) presentation of cardiac arrest, the diagnosis of PE is challenging without the use of CT angiography. Point-of-Care-Ultrasound (POCUS) is a bedside modality that can assist Emergency Physicians (EPs) in differentiating PE from other causes of cardiac arrest. Tintinalli, J.E.
In this situation, an ABG should be obtained periodically for correlation, though this is more relevant for the intensive care unit (ICU) setting than in routine ED care (5, 9). Int J Emerg Med. The role of venous blood gas in the emergencydepartment: a systematic review and meta-analysis. Eur J Emerg Med.
Background: The ongoing debate between video laryngoscopy (VL) and direct laryngoscopy (DL) has ignited intense debate within the emergency medicine and criticalcare communities. 11 medical centers in the United States enrolled 1417 patients from 17 sites, including 7 emergencydepartments and 10 intensive care units.
CriticalCare. J Emerg Med. Clinical spectrum of rhabdomyolysis presented to pediatric emergencydepartment. Int J Emerg Med. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. CriticalCare. He has no medical problems. Published June 2009.
found no difference in mortality in criticalcare patients treated with vancomycin and piperacillin- tazobactam compared to vancomycin and cefepime or meropenem. What They Did: Investigators performed a retrospective cohort study in the EmergencyDepartment at the University of Michigan between July 1, 2014 through December 31, 2018.
CriticalCare Medicine 41(12):p A191, December 2013. Intranasal fentanyl and discharge from the emergencydepartment among children with sickle cell disease and vaso-occlusive pain: A multicenter pediatric emergency medicine perspective. Roy A, Allareddy V, Lee M, Nalliah R, Rampa S, Allareddy V, Rotta A.
Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation. GBS is a clinically important diagnosis for both the emergencydepartment and the ICU. Read More » Welcome back to the tasty morsels of criticalcare podcast.
Aaron Skolnik is an Assistant Professor of Emergency Medicine at the Mayo Clinic Alix School of Medicine and Vice Chair of CriticalCare Medicine at Mayo Clinic Arizona. He is board-certified in Emergency Medicine, Medical Toxicology, Addiction Medicine, Internal Medicine-CriticalCare, and Neurocritical Care.
1] Fred is a 3-year-old boy who presents to the emergencydepartment. This is because central pressures may not always be pathologically transmitted to the organs we care about (e.g. Taken together, the adult criticalcare community has shifted towards assessing for venous congestion at the organ level with Doppler ultrasound.
Volume status Assessing volume status, especially in critically ill patients, can be challenging. Since the 2010s multiple trials have explored the feasibility of fluid restrictive resuscitation both on initial resuscitation in the ED, as well as in the intensive care unit (ICU). The rational clinical examination.
This makes it a valuable adjunct in multimodal sedation and analgesia strategies, particularly in paediatric criticalcare and procedural sedation. Dexmedetomidine is currently licensed only for adult sedation in an ICU setting, but guidelines exist to support its off-licence use in paediatric intensive care (PICU).
New and Progressive Medical Conditions After Pediatric Sepsis Hospitalization Requiring CriticalCare. but PPV ranges from 25.1-39.5% years Internal validation cohort: 43,400 patients with mean age 3.7 years External validation cohort: 45,855 patients with mean age 2.6 0.38 (95% CI 0.20-0.39) 0.39) AUROC of 0.71-0.92 0.92 (95% CI 0.70-0.92)
The value of white blood cell count in predicting serious bacterial infections in children presenting to the emergencydepartment: a multicentre observational study Archives of Disease in Childhood 2025;110:191196. Am J Emerg Med. The sepsis screening tool in paediatric emergencydepartments can help. 2025.01.054.
PECARN prediction rule for cervical spine imaging of children presenting to the emergencydepartment with blunt trauma: a multicentre prospective observational study. Lancet Child Adolesc Health. 2024 Jul;8(7):482-490. doi: 10.1016/S2352-4642(24)00104-4. Epub 2024 Jun 4.
Bend the stylet Unless youre a lunatic who likes surprises during criticalcare procedures, you should bend your own stylet. It is true, someone finally did an RTC on ICU level patients and found that first pass success IS better with VL than DL (Prekker 2023), but the fact remains that sometimes VL fails. Ann Emerg Med.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content