This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
To celebrate the end of trauma season ( is it ever really over? ), we here at the Ped EM Morsels Bakery have cooked up a morsel to remind you that pediatric trauma can be even more difficult than you think. Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Never fear.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and criticalcare as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC? first appeared on The Skeptics Guide to Emergency Medicine.
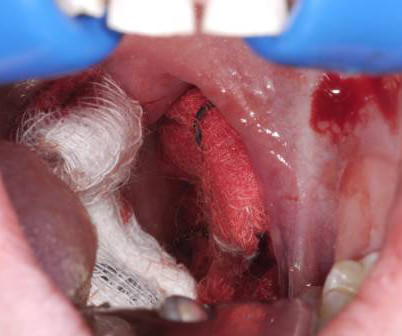
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression.
IF YOU OR A LOVED ONE NEEDS HELP, CALL 988 OR SEEK CARE AT A LOCAL EMERGENCY DEPARTMENT. WE, AS EMS PROFESSIONALS, SHALL PROVIDE COMPASSIONATE, APPROPRIATE CARE TO ALL PATIENTS. EMS must rely on the hazmat team to monitor the air and not rely on their sense of smell. CriticalCare Clinics, 39(2), 429-441.
Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a criticalcare paramedic and first year medical student at Rocky Vista University in Colorado. Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a criticalcare paramedic and first year medical student at Rocky Vista University in Colorado.
Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps. The post Post-Tonsillectomy Hemorrhage: ReBaked Morsel appeared first on Pediatric EM Morsels. Don’t await for fancy meds to arrive from pharmacy.
Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie (REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia. Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie ( REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia.
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh. 2020) The Times & Tapes Are a-Changin’: The Latest Broselow-Luten Tape for EMS , EMS World.
Critically ill patients requiring resuscitation often present with many challenges including the ability to secure safe, sterile, fast, and reliable intravenous (IV) access. Over the years emergency and criticalcare physicians have tried many ways to establish IV access in emergencies including the “crash” or “dirty” central line.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University in St. Louis); Dr. Jessica Pelletier, DO (EM Attending Physician, Washington University in St. You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Per EMS he was very cold to touch. 2009;338:b2085.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. 5 More recent literature defines “refractory” as VT or VF that is persistent or recurrent despite three shocks from a defibrillator, three rounds of epinephrine, and use of an antiarrhythmic (i.e.,
911 is called and EMS professionals are 7 minutes away. If we remove these decades old requirements we can begin to reshape human behavior at the point of care, where it matters most. In this video we describe a step by step approach to pediatric criticalcare using training that is specifically geared towards System 2 elimination.
Other Norepinephrine or epinephrine are preferred vasopressors when needed. CriticalCare Toxicology. Consider lidocaine for associated dysrhythmias. 8 Consider intravenous lipid emulsion (ILE) for cardiotoxicity not responsive to other treatments. 9-12 Do not use this prophylactically in bupropion overdoses. 2014;52(9):969-72.
EMS physicians report he was found in ventricular fibrillation. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Simon EM, Tanaka K. A 67-year-old man presents to the emergency department (ED) in cardiac arrest. He was found by bystanders after he collapsed and 911 was called.
After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. 2020), but IV Calcium is still used routinely in some cases in the criticalcare setting, such as congenital heart disease. Pediatric CriticalCare Medicine, 23 (11), 860-871. Kay, J., & Blalock, A.
Guest Skeptic: Missy Carter is a PA currently practicing in criticalcare after having attended the University of Washington's MEDEX program. Case: You’re doing a ride along with your local emergency medical service (EMS) crews and responding to an out-of-hospital cardiac arrest (OHCA). Reference: Couper et al.
Authors: Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA), Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
Earlier in the summer, I wrote a blog discussing the challenges, intricacies, and educational pitfalls of postpartum hemorrhage in EMS. In the standard care of anaphylactoid reactions, we administer Epinephrine, Diphenhydramine, steroids, and bronchodilators. CriticalCare Medicine, 33 (10), S279-S285.
Fast forward a few years, maybe a criticalcare class or a few Studio modules, and now we’ve learned that there’s a whole world of vasopressors, inotropes, inopressors, and inodilators out there. In the EMS setting, the most common cardiogenic shock patient is most likely a STEMI. mcg/kg/min. link] Levy, B., link] Shankar, A.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content