This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Consider these medications if there are signs of end-organ dysfunction, there is a considerable delta in baseline BP, systolic is less than 90 and/or MAP is less than 65 Norepinephrine is a good pressor for a lot of the situations that we encounter in the emergency department, such as septic shock, undifferentiated shock and hypovolemic shock.
Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Crystalloid may help, but neurogenic shock may not respond to fluid administration. Alpha 1 agonists are necessary to maintain appropriate blood pressure.
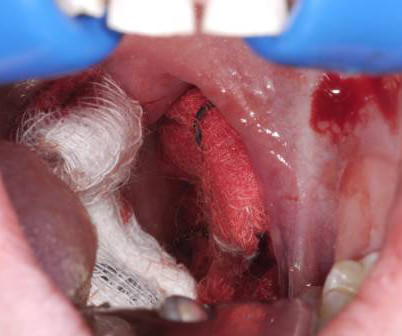
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression.
HIET improves contractility without increasing SVR, while vasopressin and epinephrine transiently increase SVR/MAP but worsen cardiac output in anesthetized dogs given propranolol (Holger 2007). Insulin versus vasopressin and epinephrine to treat β-blocker toxicity. Strong trend across different study designs for superiority of HIET.
Children who develop stridor may be treated with racemic epinephrine (0.25- 0.75ml of 2.25% racemic epinephrine to 2.5 CriticalCare Clinics, 39(2), 429-441. Consider nebulized bronchodilators for bronchospasm, using the standard cautions in their use based on the age of the patient. 2018, 05 21). 2019, 10 30).
Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a criticalcare paramedic and first year medical student at Rocky Vista University in Colorado. Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a criticalcare paramedic and first year medical student at Rocky Vista University in Colorado.
Guest Skeptic: Dr. Neil Dasgupta is an emergency physician and ED intensivist from Long Island, NY, and currently an assistant clinical professor and Director of Emergency CriticalCare […] The post SGEM#350: How Did I Get Epi Alone? Epinephrine is provided and you quickly place an advanced airway.
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps. . < 25 kg = 250 mg up to 3x > 25 kg = 500 mg up to 3x Direct Pressure Always the best way to stop bleeding. Don’t await for fancy meds to arrive from pharmacy.
We went four rounds punching and counter punching arguments about criticalcare controversies. We both agree that the patient deserves the best care, based on the best evidence. It is an example of mixing education and entertainment for some great knowledge translation. The REBEL took the fight to the Skeptic.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and criticalcare as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC? first appeared on The Skeptics Guide to Emergency Medicine.
The book Buy the new textbook (Bryan edited, Brandon authored a chapter) here or on Amazon: Concepts in Surgical CriticalCare, First Edition ed. To hemodynamically manage RV failure without worsening RV afterload, consider the Rule of 8s cocktail:* Epinephrine.08 an overly high FiO2 will tend to worsen V/Q matching.*
Research interests include simulation-based assessment, transport medicine, and criticalcare analgesia. He is an assistant professor at the Northern Ontario School of Medicine University and is passionate about health equity for rural and indigenous populations.
Pediatric Crit Care Med. 2022 Date: February 15, 2023 Guest Skeptic: Dr. Carlie Myers is Pediatric CriticalCare Attending at Cincinnati Children’s Hospital Medical Center. Pediatric Crit Care Med. Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base.
Epinephrine at lower doses is a good second line, providing inotropic support for the RV without much impact on PVR. Click here to claim your CME credit! Find us on Patreon here! Buy your merch here! . Place an arterial line early. Consider a central one such as in the femoral artery if they’re sick.
Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh. [Krug 2007] What If the Child is Obese or Emaciated? There are other systems that account for body habitus.
Critically ill patients requiring resuscitation often present with many challenges including the ability to secure safe, sterile, fast, and reliable intravenous (IV) access. Over the years emergency and criticalcare physicians have tried many ways to establish IV access in emergencies including the “crash” or “dirty” central line.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. 5 More recent literature defines “refractory” as VT or VF that is persistent or recurrent despite three shocks from a defibrillator, three rounds of epinephrine, and use of an antiarrhythmic (i.e.,
Be aggressive with fluid resuscitation and consider epinephrine up to 0.06–0.08 .* Adding an inotrope can be somewhat diagnostic, as patients with mere myocardial stunning will improve, whereas patients with tamponade will generally have little response.* Give calcium chloride freely to the unstable post-cardiac surgery patient.*
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/criticalcare pod of your emergency department (ED). The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field.
If we remove these decades old requirements we can begin to reshape human behavior at the point of care, where it matters most. In this video we describe a step by step approach to pediatric criticalcare using training that is specifically geared towards System 2 elimination. What changed?
After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. 2020), but IV Calcium is still used routinely in some cases in the criticalcare setting, such as congenital heart disease. Pediatric CriticalCare Medicine, 23 (11), 860-871. Kay, J., & Blalock, A.
Epinephrine Shock (any) Cardiac arrest Bronchospasm Anaphylaxis Bradycardia (second-line alternative) Infusion : 0.01 Effects of dopamine, norepinephrine, and epinephrine on the splanchnic circulation in septic shock: which is best? Crit Care Med 2003; 31:1659. Use of inotropes in the criticalcare setting.
However, the decade since the original Hypothermia after Cardiac Arrest trial had seen significant advances in pre-hospital, emergency department, and criticalcare that may have contributed to these outcomes. These results suggest that targeting a lower temperature of 33ºC confers no additional benefit to targeting 36ºC.
Crit Care Med. 1991 May;19(5):694-9 Objective: To evaluate the efficacy and safety of potassium replacement infusions in critically ill patients. Setting: Multidisciplinary criticalcare unit. Design: Prospective cohort study. mmol/L (n = 26), 3.0 The incidence of hypokalemia (potassium less than 3.5
Other Norepinephrine or epinephrine are preferred vasopressors when needed. CriticalCare Toxicology. Consider lidocaine for associated dysrhythmias. 8 Consider intravenous lipid emulsion (ILE) for cardiotoxicity not responsive to other treatments. 9-12 Do not use this prophylactically in bupropion overdoses. 2014;52(9):969-72.
Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. A 67-year-old man presents to the emergency department (ED) in cardiac arrest. He was found by bystanders after he collapsed and 911 was called. EMS physicians report he was found in ventricular fibrillation.
Guest Skeptic: Missy Carter is a PA currently practicing in criticalcare after having attended the University of Washington's MEDEX program. The paramedic is trying to get intravenous (IV) access to give epinephrine per the protocol. Epinephrine has long been a cornerstone in the management of OHCA.
If you’re above this DBP, just skip epinephrine, which will probably merely be toxic (ie promoting arrhythmias). * Finally, if it’s truly just vasoplegia, consider other moves, such as adding vasopressin/steroids (an evidence-based practice) or high-dose epinephrine (5 mg epinephrine).
CriticalCare Ultrasound in Shock: A Comprehensive Review of Ultrasound Protocol for Hemodynamic Assessment in the Intensive Care Unit. EPINEPHRINE-INUDCED SHOCK: LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION ON VASOPRESSORS. m/s)—problematic and elevated > 50 mm Hg (2.5 J Thorac Dis. 2015;7(9):E365-E369. J Clin Med.
Consultation needed for definitive management: Pulmonology/criticalcare, IR, and cardiothoracic surgery; admission to the criticalcare setting (likely requires transfer). Bronchoscopy can be used for bleeding control with cold saline, epinephrine, activated factor VIIa, or TXA.
In the standard care of anaphylactoid reactions, we administer Epinephrine, Diphenhydramine, steroids, and bronchodilators. Sure, we still do CPR, defibrillate as needed, and give Epinephrine based upon our local guidance. CriticalCare Medicine, 33 (10), S279-S285. Could this work for the AFE patient?
Fast forward a few years, maybe a criticalcare class or a few Studio modules, and now we’ve learned that there’s a whole world of vasopressors, inotropes, inopressors, and inodilators out there. Low-dose epinephrine is a strong beta-1 drug with minimal alpha-1 effects if you stay below ~0.08 mcg/kg/min. link] Levy, B.,
PMID: 38857847 Bottom line: This before and after study demonstrates an association between early IM epinephrine and survival from cardiac arrest. PMID: 38857847 Bottom line: This before and after study demonstrates an association between early IM epinephrine and survival from cardiac arrest. Resuscitation. 2024 Aug;201:110266.
Methodology: 4/5 Usefulness: 3/5 Couper K, et al. N Engl J Med. 2024 Oct 31:10.1056/NEJMoa2407780. Question and Methods:This multi-center, open label randomized control trial aimed to assess 30-day survival in patients with out of hospital cardiac arrest (OOHCA) who received IO versus IV access first.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content