This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Supportive Care Intensive monitoring, often in an ICU setting. We discuss the recognition and treatment of necrotizing fasciitis. Types of Necrotizing Fasciitis Type I (Polymicrobial) Involves aerobic and anaerobic organisms (e.g., Bacteroides, Clostridium, Peptostreptococcus). diabetes, peripheral vascular disease).
The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” They are on the phone asking you if you already have another admission for them on this busy day.
Caleb Lin Hyperbaric Oxygen for the ICU Patient OVERVIEW INTENSIVE CARE INDICATIONS PRACTICAL ISSUES IN CRITICALCARE Consideration & Prior to Treatment In the Chamber A: ETT cuff to be filled with sterile water or connected to dynamic cuff inflator B: Titrate ventilation to PaCO2, note that EtCO2 is not linearly proportionate at higher pressures (..)
Aaron Skolnik is an Assistant Professor of Emergency Medicine at the Mayo Clinic Alix School of Medicine and Consultant in the Department of CriticalCare Medicine at Mayo Clinic Arizona. He is board certified in Emergency Medicine, Medical Toxicology, Addiction Medicine, Internal Medicine-CriticalCare, and Neurocritical Care.
set out to explore in the Kids THRIVE study investigating whether NHF apnoeic oxygenation could improve intubation outcomes in critically unwell children needing emergency airway management. Patients were randomised in a 1:1 ratio to receive either nasal high-flow or standard care. Thats exactly what Shane George et al.
The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. It was found that patients exposed to deep sedation in the ED had an independent higher incidence of continued deep sedation on ICU day one ( Fuller, 2019 ).
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast. Takeaway lessons * When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU. When a sending provider (e.g.
Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. Aaron Skolnik is an Assistant Professor of Emergency Medicine at the Mayo Clinic Alix School of Medicine and Consultant in the Department of CriticalCare Medicine at Mayo Clinic Arizona. Lactated Ringer’s or Plasmalyte 148) over 0.9%
Welcome back to the tasty morsels of criticalcare podcast. Part 1 will cover a broad overview of pulmonary hypertension and part 2 will focus on management strategies for a PH patient in the ICU. This time we’re looking at pulmonary hypertension. We’re going to try it as a 2 parter. This is by far the commonest.
How to manage the intubated critically ill patient while keeping them awake, non-delirious, and mobile, with Dr. Dale Needham, FCPA, MD, PhD. Dr. Needham is a Professor of Pulmonary and CriticalCare Medicine as well as Physical Medicine and Rehabilitation at the Johns Hopkins University. More fentanyl is often needed early on.
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association (AHA) and Neurocritical Care Society (NCS) released their 2023 Scientific Statement on the criticalcare management of post ROSC patients. Instead, target 92-98%. Keep hemoglobin > 7 g/dL. Treat seizures if present.
An overview of the role and contributions of a clinical pharmacist in the ICU, with Laura Means Ebbitt of the University of Kentucky, a clinical pharmacist specializing in colorectal/ENT surgery and criticalcare. Takeaway lessons A clinical pharmacist is a “knowledge pharmacist,” dispensing advice rather than medications.
Emily Fridenmaker (@emily_fri), pulmonologist and intensivist at Charleston Area Medical Center in West Virginia. Continuing education for this episode CME credit provided courtesy of Academic CME. can be elevated by diuresis* Serum albumin/pleural > 1.2* Pleural LDH/serum LDH > 0.6* glucose <40 (or 60?) glucose <40 (or 60?),
The Effect of Vitamin C on Clinical Outcome in Critically Ill Patients: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. CriticalCare Medicine. The Effect of Vitamin C on Clinical Outcome in Critically Ill Patients: A Systematic Review with Meta-Analysis of Randomized Controlled Trials.
ClinicalTrials.gov: NCT02517489 7 Clinical Question: In adult patients with severe community-acquired pneumonia admitted to the ICU, does early hydrocortisone treatment, compared to standard therapy, reduce mortality at 28 days? Patients enrolled from 31 Intensive Care Units in France. in the hydrocortisone group vs. 11.9%
We discuss the field of rehabilitation psychology, and how it can help patients with persistent critical illness, with Dr. Megan Hosey (@DrMeganHoseyPhD), clinical psychologist and assistant professor at Johns Hopkins School of Medicine, where she practices in the medical ICU. Delirium often dominates the patient experience of the ICU.
Welcome back to the tasty morsels of criticalcare podcast. This segues relatively nicely into a section of the document on palliative care. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life. With me so far?
A brief overview and call to arms around the key concepts of ICU liberation. A brief overview and call to arms around the key concepts of ICU liberation.
Welcome back to the tasty morsels of criticalcare podcast. So, from the ultra broad topic of AKI in the last podcast to the super specific question of when we should pursue an open lung biopsy in an ICU patient. Read More » Welcome back to the tasty morsels of criticalcare podcast.
Welcome back to the tasty morsels of criticalcare podcast. Vasopressin has some animal data suggesting it causes less rise in PVR than our beloved noradrenaline but take that with an appropriately loosely defined portion of salt given that animal data is not ICU patients. In terms of monitoring should we be reaching for a PAC?
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. With both ER and ICU experience, this post acts as a quick […] The post Mechanical Ventilation Basics appeared first on EMOttawa Blog.
Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Pediatric Crit Care Med. 2022 Date: February 15, 2023 Guest Skeptic: Dr. Carlie Myers is Pediatric CriticalCare Attending at Cincinnati Children’s Hospital Medical Center.
Welcome back to the tasty morsels of criticalcare podcast. Oh Chapter 37 is dedicated to NIV in the ICU and is probably worth some time given that this is a common respiratory support both in the ICU and throughout the hospital. On an ICU vent this would be described as 5/5. Still to be proven but commonly tried.
Stephanie Martin (Twitter: @OBCriticalCare, Instagram: @criticalcareob), medical director for Clinical Concepts in Obstetrics and a Maternal Fetal Medicine specialist in Scottsdale, Arizona with expertise in criticalcare obstetrics. She is also co-host of the CriticalCare Obstetrics podcast. This is not the goal.*
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. This is a mammoth topic that listening to 5 mins of me rambling will in no way seriously prepare you to either practice clinically or write a semi coherent exam. That being said here we go.
Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation. HIV in the ICU is becoming a bit of a rare beast as the ID docs seem to have it so. Read More » Welcome back to the tasty morsels of criticalcare podcast.
Takeaway lessons * Invasive aspergillosis is among the most common diseases identified on autopsy studies of ICU patients that was not recognized prior to death. Infection in the ICU patient arises when there are abnormalities in the flow of fluid, anatomical barriers, and/or the immune defenses (particularly neutrophil function).*
Conservative versus liberal oxygenation targets in critically ill children (Oxy-picu): a UK multicentre, open, parallel-group, randomised clinical trial. Dr. Anireddy Reddy Case: A 3-year-old girl presents to the emergency department (ED) with fever and respiratory distress. But like many interventions, there are potential harms and benefits.
Signs of baseline and/or new RV strain, such as reduced TAPSE, septal bowing, etc, as well as pericardial effusion, suggest a poor reserve for the stresses of their new ICU course. Click here to claim your CME credit! Find us on Patreon here! Buy your merch here! Non-invasive cardiac output monitors are of questionable utility. *
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. However in ICM there is a need to have a broad understanding of what some of the haematological acronyms might mean given that a fair number of these patients end up in the ICU.
The art of taking a critically ill, heavily sedated, floridly delirious patient on aggressive vent support and pulling them out of the loop of sedation, immobility, and delirium. A spiritual successor to our talk with Dale Needham , this time focusing more on details and practical approaches. .* Limited activity is better than none.
Welcome back to the tasty morsels of criticalcare podcast. As an EM trainee doing intensive care I will confess that I struggle to work up the enthusiasm to cover a nutrition guideline. Read More » Welcome back to the tasty morsels of criticalcare podcast. As with all ICU nutrition EN is preferred over PN.
Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation. Read More » Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation.
Welcome back to the tasty morsels of criticalcare podcast. The major barrier to implementation in the ICU setting is the almost complete absence of ICU patients from these trial cohorts. Welcome back to the tasty morsels of criticalcare podcast. Many penumonias will develope a parapneumonic effusion.
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. After 2 years of frequent, if not daily use of the bronch, I find it hard to see how I would manage in an ICU without it. Why might we pull out the bronch in the ICU?
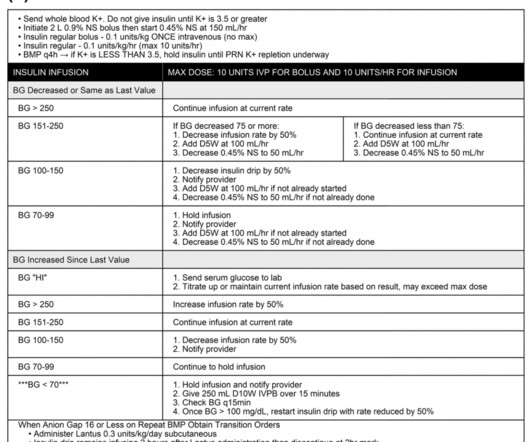
Disposition to ICU. Experts consensus recommendations for the management of calcium channel blocker poisoning in adults: CriticalCare Medicine. Supplement additional dextrose prn, if hypoglycemia occurs do not stop the insulin, increase the rate of the dextrose drip. References: Yuan TH, Kerns WP, Tomaszewski CA, et al.
Back in the arena with one of our favorites, Matt Siuba (@msiuba), Cleveland Clinic intensivist and Mr. Zentensivism, to discuss complications in criticalcare and how to prevent and manage them. Takeaway lessons * Rapid atrial fibrillation in the ICU should be considered a “symptom,” not a disease per se.
A look at oncology-related emergencies in the ICU, with Leon Chen (@CCMNP), NYC nurse practitioner specializing in oncology criticalcare. This can be resolved with whole blood samples or point-of-care assays, which decrease transport time and sample agitation.* Pulse oximetry is more reliable.*
In our emergency department, the RTs do not spend a lot of time going around measuring cuff pressures and usually save that until the patient reaches the ICU. Another minor difference is that the gastric balloon in the Minnesota tube holds 450-500 ccs of air, while the SB gastric balloon holds 250 ccs of air [2].
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. We all get excited about CMV but in reality this is not often an ICU issue in the post transplant period and comes later on often at the 3-4 week mark. Part 1 lives here.
Welcome back to the tasty morsels of criticalcare podcast. It is with trepidation that I approach any topic that involves the negative feedback loops of endocrine control as I really struggle to keep it all straight in my head, Read More » Welcome back to the tasty morsels of criticalcare podcast.
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. Like most spaces within the body, the contents within the cranium are under a certain degree of pressure. The skull being a rigid box can accommodate pressure much less than.
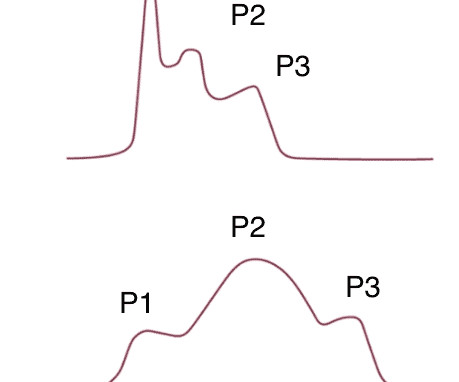
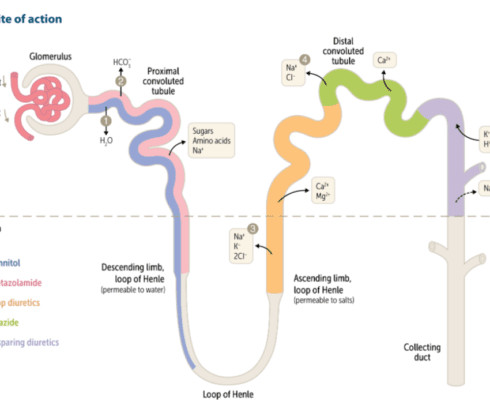
Welcome back to the tasty morsels of criticalcare podcast. Today we’re going to talk about some of the basics of some of our favorite drugs intensive care – the diuretics. As always this is planned to be a brief overview of the essentials rather than the deep dive. Lose the Na and the water will follow.
Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation. Today’s podcast is mostly taken from Oh’s manual Chapter 96 covering criticalcare nutrition. Read More » Welcome back to the tasty morsels of criticalcare podcast.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content