This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
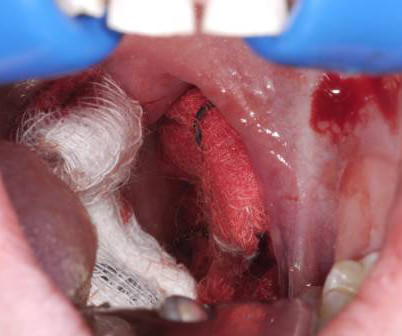
The literature suggests that approximately 85 percent of these cases require procedural source control in the operatingroom, highlighting the importance of expediting transport arrangements. Secondary post-tonsillectomy hemorrhages often require surgical intervention.
As such it has enjoyed widespread adoption throughout the Emergency Medicine and CriticalCare world. There have been some studies in various clinical settings (operatingroom, criticalcare and pre-hospital) that have demonstration benefit of apneic oxygenation.
They concluded that propofol is safe, particularly in short-term sedation, but should be used with caution outside of the operatingroom, given some of the potentially severe adverse events (including PRIS) seen. Only one of these studies was undertaken in an intensive care setting, and it did not report any cases of PRIS.
Welcome back to the tasty morsels of criticalcare podcast. A meandering monologue through criticalcare fellowship exam preparation. Oh’s Manual chapter 104 has a decent chapter on the intensive care aspects of lung transplant. Read More » Welcome back to the tasty morsels of criticalcare podcast.
Takeaway lessons * Trauma patients who are hypotensive or otherwise unstable should be assumed to be bleeding, bleeding, bleeding until proven otherwise, and should have a very low threshold to proceed directly to the operatingroom for exploration.*
Am J Emerg Med. 2016; PMID: 27720568 Guest Post By: Courney Knieriem, MD PGY-1, Emergency Medicine Resident RWJBH Community Medical Center, Toms River, NJ Courtneyknieriem.md@rutgers.edu
In our case, the patient had a CT of the head, cervical spine, and chest, abdomen, and pelvis with intravenous contrast demonstrated a C2, C7 compression fracture with significant bowel edema (Figure 4), and was taken to the operatingroom for left arm disarticulation, left below knee amputation and right above knee amputation.
This is a critical error that leads to poorer outcomes for patients in need of criticalcare. As volumes increase of patients actively being worked up is paired with those who need eventual admission, there is a higher task burden which creates a significant barrier to adequate criticalcare delivery.
A search for Brazilian Butt Lift (BBL) on any social media platform will yield thousands of before-and-after images, faja sales, operatingroom videos, recovery tips, and patients praising their plastic surgeon. References Garcia SE. Butt Lifts Are Booming. Healing Is No Joke. The New York Times.
Students must complete a minimum of 250 hours of clinical experience in the hospital setting including the emergency room, operatingroom, and labor and delivery. This is followed by 250 hours of clinical externship, also called “ride time”, on an ambulance under the supervision of a licensed paramedic.
Video Laryngoscopy vs Direct Laryngoscopy for Endotracheal Intubation in the OperatingRoom: A Cluster Randomized Clinical Trial. Position Paper on the Reporting of Norepinephrine Formulations in CriticalCare from the Society of CriticalCare Medicine and European Society of Intensive Care Medicine Joint Task Force.
Oppositely, if the patient is not suffering from cardiac arrest, I would still encourage you to move with haste but try to transport the patient to a hospital with an in-house obstetrician and operatingroom capabilities, while notifying the hospital as early as possible. CriticalCare Medicine, 33 (10), S279-S285.
Bend the stylet Unless youre a lunatic who likes surprises during criticalcare procedures, you should bend your own stylet. ” Australian CriticalCare 20.4 “Effect of cooling on oxygen consumption in febrile critically ill patients.” ” Annals of Intensive Care 10 (2020): 1-9. .
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content