This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post Ep 169 Cardiac Arrest Controversies – Chest Compressions, Dual Defibrillation, Medications and Airway appeared first on Emergency Medicine Cases.
You continue with compressions and defibrillations and your partner places an advanced airway. The patient is a 54-year-old man who collapsed in front of his family after complaining of chest pain for several hours. On your arrival, first responders from the fire department are performing high-quality basic cardiac life support.
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Further information is not available.
Defibrillation Strategies for Refractory Ventricular Fibrillation. Defibrillation Strategies for Refractory Ventricular Fibrillation. He has been an ACLS instructor for close to 30 years and notably his first publication focused on out-of-hospital defibrillation. Defibrillation Strategies for Refractory Ventricular Fibrillation.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation? 2,3 Multiple published studies have addressed treatment of ventricular fibrillation with defibrillation and medications such as amiodarone and lidocaine.
St.Emlyn's - Emergency Medicine #FOAMed This secondary analysis of the DOSE VF trial highlights double sequential external defibrillation (DSED) as a superior strategy over standard and vector change defibrillation for refractory ventricular fibrillation (RVF) in out-of-hospital cardiac arrest, improving survival rates and neurological outcomes (..)
Sarah Reid on pediatric appendicitis risk calculator, Sheldon Cheskes & Mark Ramzy on double defibrillation for refractory ventricular fibrillation, Hans Rosenberg & Krishan Yadav on cellulitis clinical pearls, Anand Swaminathan on serratus anterior block, Brit Long on recognition of toxic shock syndrome, Justin Morgenstern on tranexamic acid (..)
We should focus more on high-quality CPR and early defibrillation for shockable rhythms and less on type of supraglottic airway device. The SGEM has also covered prehospital intubation using supraglottic devices for out-of-hospital cardiac arrests (OCHAs) with PA Missy Carter ( SGEM#247 and SGEM#396 ).
A recent case has highlighted the extraordinary potential of a novel intervention: triple-sequential defibrillation. The Case Unfolds Despite 82 minutes of high-quality CPR and Advanced Cardiovascular Life Support (ACLS) management, standard and dual-sequential defibrillation failed to restore the patient’s heartbeat.
This is because of the ease of finding anatomic landmarks and their location away from other procedures like defibrillation, CPR, and airway management. The classic location for IO placement is the tibial plateau.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
In this CritCases blog Michael Misch takes us through a case of accidental hypothermia and cardiac arrest, reviewing the controversies in management as well as the guidelines for rewarming, the role of ECMO and the alterations to ACLS cardiac arrest medications, CPR and defibrillations.
You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive. Unfortunately, most patients don’t receive these crucial interventions.
This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. Background: We have covered Out of Hospital Cardiac Arrests (OHCAs) many, many times on the SGEM.
St.Emlyn's - Emergency Medicine #FOAMed Should we use AP or AL pad position first for defibrillation in VF/VT cardiac arrest. Critical appraisal of an observational study in JAMA suggests a better outcome with AP, but there are many biases in this study. FOAMed @stemlyns The post JC: AP or AL pad position for first choice shock in VF?
3: Does Defibrillator Pad Placement Matter for OHCA? Source Initial Defibrillator Pad Position and Outcomes for Shockable Out-of-Hospital Cardiac Arrest. Source Emergency Department Blood Pressure Treatment and Outcomes in Adults Presenting with Severe Hypertension. West J Emerg Med. 2024;25(5):680-689. #3: JAMA Netw Open. 2024.31673.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. This patient was witnessed by bystanders to collapse. They started CPR. EMS arrived and found him in Ventricular Fibrillation (VF).
Spoon Feed This secondary analysis of the DOSE VF trial found that DSED (dual sequence external defibrillation) was the superior strategy for obtaining ROSC and functional neurologic outcome regardless of whether the patient was in recurrent VF or shock-refractory VF after three standard defibrillation shocks.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. Much depends on the post resuscitation ECG and its evolution shortly after defibrillation. Does this patient have ACS? Should he necessarily go to the cath lab?
One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. We now know that an emphasis on the basics (high quality chest compressions and defibrillation) are the most important aspects of resuscitation. Case: A 46-year-old man has a cardiac arrest at home, witnessed by family.
Bystander high-quality CPR can buy you some time until defibrillation. We know that rapid application of electricity to defibrillate shockable arrhythmias save lives. There are five steps in the Chain-of-Survival for OHCA: Most of us can agree with the first three steps. You need to recognize an arrest and activate your EMS system.
A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. Case: A 51-year-old man experiences a cardiac arrest on the street. You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). He is unsuccessfully shocked.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
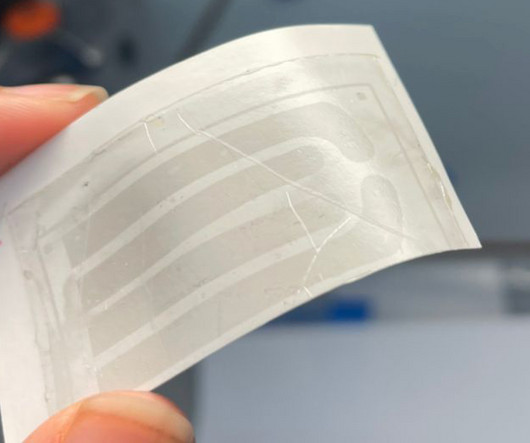
“All of the cells inside the heart get hit at one time, including the pain receptors, and that’s what makes pacing or defibrillation painful,” said Philipp Gutruf, a researcher involved in the study. Moreover, when electrical signals are sent to the heart, every cell receives the shock, often leading to pain and discomfort.
A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Case: A paramedic crew responds to a 54-year-old male in cardiac arrest at a private residence.
4: VF or VT – Earlier Defibrillation Is Better? Source The impact of time to defibrillation on return of spontaneous circulation in out-of-hospital cardiac arrest patients with recurrent shockable rhythms. Source Management of Pustules and Vesicles in Afebrile Infants ≤60 Days Evaluated by Dermatology. Pediatrics. doi: 10.1542/peds.2023-064364.
“One of the challenges for current pacemakers and defibrillators is that they are difficult to affix onto the surface of the heart,” said Igor Efimov, one of the creators of the new technology. “Defibrillator electrodes, for example, are essentially coils made of very thick wires.
University of Maryland Department of Emergency Med
NOVEMBER 7, 2022
DOSE VF (DOuble SEquential External Defibrillation for Refractory VF) Trial Background - High quality data regarding the use of. Click to view the rest
We also gave insulin and furosemide (which take much longer to have their effect) After episodes of asystole and VF with defibrillation, she obtained ROSC and this 12-lead was recorded: The monitor around this time was NOT showing a very wide complex What do you think? How would you treat?
Measures of ventilation rates, singular tidal volume and one-minute volume were taken for comparison against international recommendations. Results: The SMART and Adult BVM mean ventilation rates were within recommended guideline parameters (i.e., 10–12 BPM).
With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. Consider administering epinephrine after defibrillation in those with shockable rhythms. COR 2b, LOE C-LD. COR 3, No benefit, LOE B-R. COR 2b, LOE B-R. COR 2b, LOE C-LD.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. The septum is punctured with the active fixation screw of the lead - so essentially you bore the septum with the screw helix."
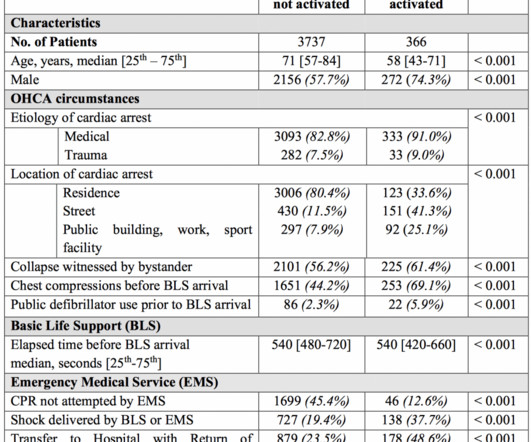
OHCA was defined as persons found apneic and without a pulse who underwent either external defibrillation (bystanders or EMS) or chest compressions. JAMA 2020 * Population: Adults 18 years and older with non-traumatic OHCA between 2011 and 2015treated by 192 EMS agencies in the USA.
Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Background: The American Heart Association estimates there are approximately 350,000 EMS-assessed out-of-hospital cardiac arrests (OHCAs) in the United States per year.
Early CPR plays an important role in the American Heart Associations (AHA) Chain of Survival , which emphasizes recognizing symptoms quickly, activating 911, performing CPR, and practicing early defibrillation and post-resuscitation care.
2 If Torsade de Pointes develops, defibrillate the patient if unstable, give magnesium, and consider overdrive pacing. If the EKG is normal in an asymptomatic patient at 6 hours, there is low likelihood of cardiac complication. 1 If the EKG is abnormal or patient continues with AMS at 6 hours, admit for cardiac monitoring for 24 hours.
Paramedics managed to get return of spontaneous circulation after a single defibrillation, but the patient is still comatose on arrival. When paramedics arrived, they found him to be in cardiac arrest, with ventricular fibrillation on the monitor. The charge nurse turns to you and asks: should I grab the ice packs?
Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base. A team member asks if you want to administer some sodium bicarbonate (1mEq/kg). Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content