This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. After 1 mg of epinephrine they achieved ROSC.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
On arrival to the ED, this ECG was recorded: What do you think? Although one may have all kinds of ischemic findings as a result of cardiac arrest (rather than cause of cardiac arrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. The April 8, 2022 post by Drs.
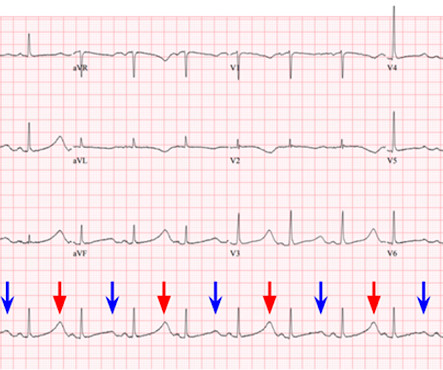
They are not premature, by definition. We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Chou’s Electrocardiography in Clinical Practice (6th ed). The green arrows, however, do show premature complexes. Question 2: What explains the conduction abnormalities? Surawicz, B.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. On arrival to the ED the patient was intubated with normal vital signs. E lectrical A lternans : Definition/Features/Mechanisms Electrical alternans — is a beat-to-beat variation in any one or more parts of the ECG recording.
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? The 4th universal definition mentions ST depression, posterior MI, and T-wave changes."
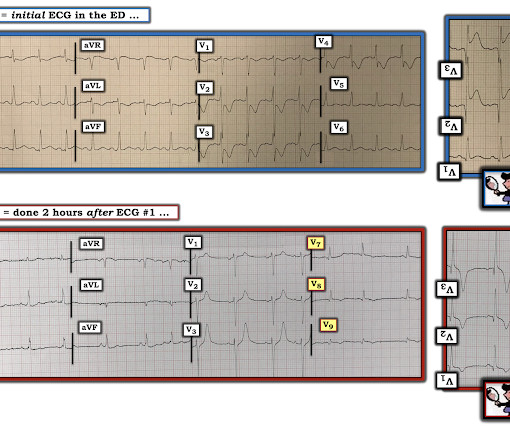
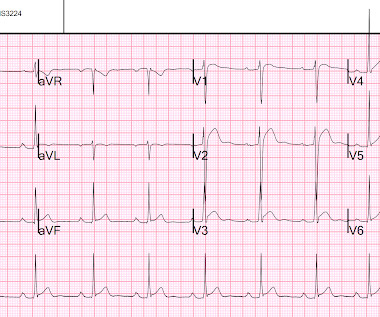
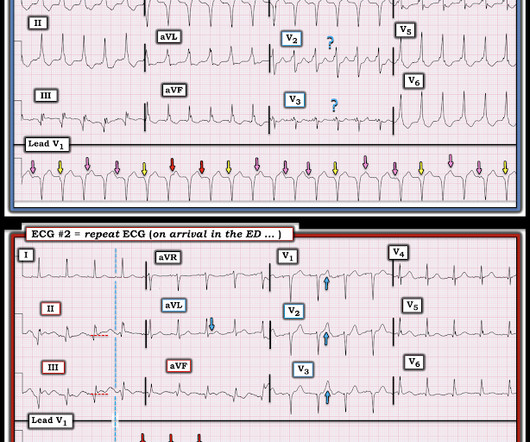
So this is a normal amount of STE in V2 and V3, defined by Universal Definition of MI as up to 2.0 So there is definitely no STEMI, and the STE is normal. Defibrillated out of v fib in the cath lab. For clarity — I’ve labeled a number of KEY findings in the initial ECG performed in the ED ( = E CG # 1 in Figure-1 ).
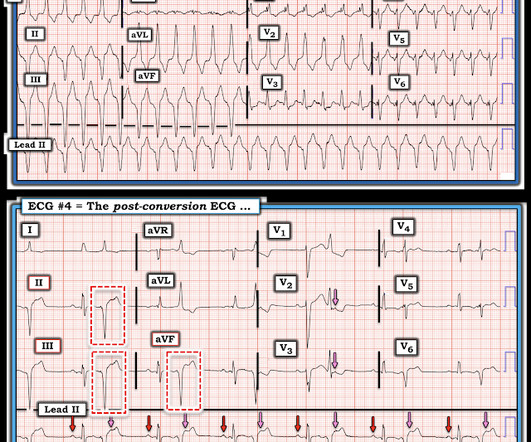
She was never defibrillated. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. The ultimate reason for the long QT was never definitively determined. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). What do you think?
If the patient only had these two ECGs recorded, it would have missed the transient time between them which were STEMI positive, and the patient would then have arrived at the ED as “serial ECGs STEMI negative." There was 100% proximal LAD occlusion, EF was 55% with severe hypokinesis to mid-distal septum and apex.
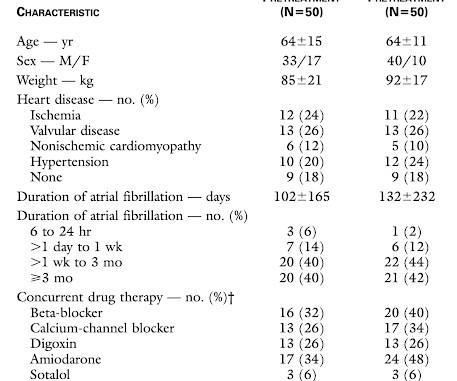
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. Methods. . = 25, 2022 ).
She was defibrillated and resuscitated. To Emphasize: The reason definitive diagnosis is important in today's case — is that the senior ED physician interpreted ECG #1 as "nothing too exciting". Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. But as it was, the delay to defibrillation was not long and it may be that nothing could have saved him.
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergency department, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
Rhythm B: This patient was seen in the ED — and thought to be in AFlutter with 4:1 AV conduction. Rhythm C: This telemetry strip from an older adult was initially thought to need defibrillation. Rhythm A: This rhythm strip was observed on telemetry — and thought to be AFlutter.
Only 5-18% of ED patients with chest pain have a myocardial infarction of any kind. Cardioversion/defibrillation. Could this be a coincidence that the patient was experiencing chest pain and upon ECG capture the atypical brugada pattern was found? Answer : History is insensitive and nonspecific. It helps a little bit. Hypothermia.
-- Comment by K EN G RAUER, MD ( 1/30/2019 ): -- Superb presentation and discussion by Dr. Alexandra Schick ( with edits by Dr. Smith ) of an elderly woman who was seen in the ED for altered mental status, hyperthermia, and the initial ECG shown above.
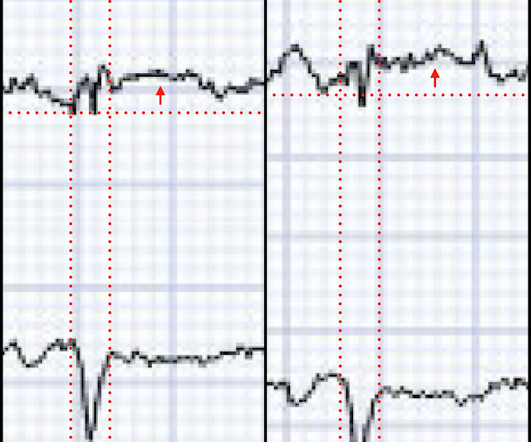
Treatment is by ICD ( implantable cardioverter defibrillator ). Regarding ECG #1 — I chose the lead with the most ST-T wave deviation ( = lead V2 in Figure-1 ) to draw in 2 vertical BLUE lines highlighting the point where I thought definite “peaking of the T wave" is seen.
On arrival in the ED, a bedside ultrasound showed poor LV function (as predicted by the Queen of Hearts) with diffuse B-lines. We rapidly defibrillated her, and with return of normal sinus rhythm. Several minutes later the patient developed V-fib again > 200J defibrillation with return to NSR. She was given 2 mg Magnesium.
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. In other words, millimeters really don't matter!
Fortunately , you don't need to make a definite diagnosis. Second , when you have a rhythm problem, you are likely to be able to fix the problem with electricity (cardioversion, defibrillation, pacing). Making a specific ECG Diagnosis (less important in the ED) Without reading the below, I suspected posterior fascicular VT.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content