This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
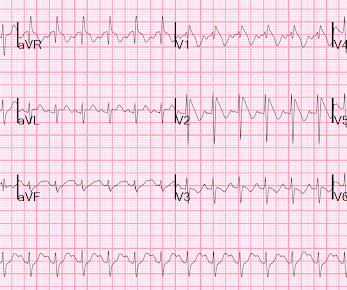
Her first set of vitals were documented: BP 116/57 Pulse 94bpm Respiratory rate 24/min O2 sat 90% on room air Temp 97F She had been cleaning a Jeep in the sun, and was sunburned. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. The physician documented “normal sinus rhythm”.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. In both tracings — an exceedingly fast PMVT is documented.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrial fibrillation.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B ECG monitoring should start immediately and a defibrillator must be ready.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 How would you treat? I could find very little literature on the treatment of severe life-threatening hypokalemia. "If If the patient is at 1.8,
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Implantable Cardioverter-Defibrillator ), with long-term potential for device-related complications from the ICD, including inappropriate shocks? Bayes de Luna, A et al.
The note documents that the first view of the LCX showed 99%, TIMI 2 flow, but then (before intervention) was seen to fully occlude in real time (100%, TIMI 0). Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. Documentation does not indicate whether she had persistent chest pain during this time. It is almost certainly not acute.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content