This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Further information is not available.
When emergency department (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. This is because of the ease of finding anatomic landmarks and their location away from other procedures like defibrillation, CPR, and airway management. The classic location for IO placement is the tibial plateau.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. He was found by bystanders after he collapsed and 911 was called.
Spoon Feed This secondary analysis of the DOSE VF trial found that DSED (dual sequence external defibrillation) was the superior strategy for obtaining ROSC and functional neurologic outcome regardless of whether the patient was in recurrent VF or shock-refractory VF after three standard defibrillation shocks. PMID: 38522736. #2:
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Here is the initial ED ECG. What do you think?
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. After 1 mg of epinephrine they achieved ROSC.
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. A middle-aged male had a V Fib arrest. He had a history of CAD with CABG.
2 If Torsade de Pointes develops, defibrillate the patient if unstable, give magnesium, and consider overdrive pacing. In: Nelson LS, Howland MA, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS, eds. His roommate found an empty pill bottle on the floor next to him. 1,2 Consider lidocaine if sodium bicarbonate fails. 1 Class IA (e.g.,
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
Early CPR plays an important role in the American Heart Associations (AHA) Chain of Survival , which emphasizes recognizing symptoms quickly, activating 911, performing CPR, and practicing early defibrillation and post-resuscitation care. You can also measure and monitor symptoms using the clinical opiate withdrawal scale (COWS).
Case: A 6-month-old boy presents to the emergency department (ED) with three days of worsening cough, cold symptoms, and fever. Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU). Pediatric Crit Care Med. Parents note that he has been progressively more tired and difficult to arouse.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
Case: During a busy emergency department (ED) shift the paramedic phone rings. OHCA was defined as persons found apneic and without a pulse who underwent either external defibrillation (bystanders or EMS) or chest compressions. CPR is currently in progress with a single shock having been delivered.
He has been taking increased doses of torsemide without improvement in his symptoms and was directed to the ED for inpatient therapy. Now, a remote outpatient pulmonary arterial pressure monitor and other heart failure detection devices (Table 1) are available that you may begin to see in your ED.
This post will focus on the key parts of the guideline that affect ED evaluation and management. With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. COR 2b, LOE C-LD. COR 3, No benefit, LOE B-R. COR 2b, LOE B-R.
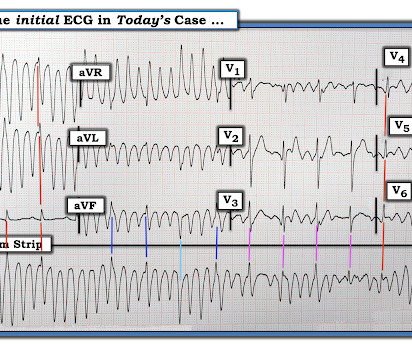
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility. The LCX was noted to be "subtotally stenosed" at the time of cath.
Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform. A simplified standard protocol for ED management is below 3. The patient is awake and protecting her airway.
Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Anyone who has worked emergency medicine for any length of time immediately recognizes this statement as a cry for help and equally portends dire change. He became unconscious as the monitor displayed VF.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Dr. Rad is ED faculty at Wellstar Kennestone Regional Medical Center in Marietta, Ga., Click to enlarge.) and at Naples Community Hospital in Naples, Fla.
On arrival to the ED, this ECG was recorded: What do you think? Although one may have all kinds of ischemic findings as a result of cardiac arrest (rather than cause of cardiac arrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Chou’s Electrocardiography in Clinical Practice (6th ed). Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. Circulation, Vol 139, No 16, 1974-76.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. On arrival to the ED the patient was intubated with normal vital signs. By EMS report, open pill bottles were found nearby at the scene, including quetiapine, fluoxetine, hydroxyzine, and gabapentin.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
Here is his ECG on presentation to the ED, approximately 45 minutes after onset of pain, but with pain improving since onset: What is your interpretation? The initial ECG was interpreted as "normal" by the computer ( Algorithm: Marquette GE / 12SL ) and "no acute ischemic changes" by the ED physician.
Submitted by Dr. Arjun J V in India, An elderly patient presented to the ED with multiple complaints. As worrisome as the initial recording in leads I and II look — a glance at lead III should immediately reassure us that defibrillation is not needed! An ECG was recorded in triage: What do you think?
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? The patient was defibrillated, and then taken to the nearest ED where ECG #1 was obtained ( Figure-1 ).
She was never defibrillated. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). As was seen in this case — defibrillation and/or overdrive pacing may be needed.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. A healthy 45-year-old female presented with chest pain, with normal vitals.
Defibrillation Strategies for Refractory Ventricular Fibrillation. So please, sit back relax, have a quiet drink and enjoy some of the nerdiest medical podcasting out there. DOSE VF: Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. N Engl J Med. 2022 Nov 6.
Defibrillated out of v fib in the cath lab. For clarity — I’ve labeled a number of KEY findings in the initial ECG performed in the ED ( = E CG # 1 in Figure-1 ). Figure-1: The initial ECG done in the ED ( See text ). "Bedside echo revealed anteroseptal wall motion abnormality at which point I activated a code STEMI.
If the patient only had these two ECGs recorded, it would have missed the transient time between them which were STEMI positive, and the patient would then have arrived at the ED as “serial ECGs STEMI negative." There was 100% proximal LAD occlusion, EF was 55% with severe hypokinesis to mid-distal septum and apex.
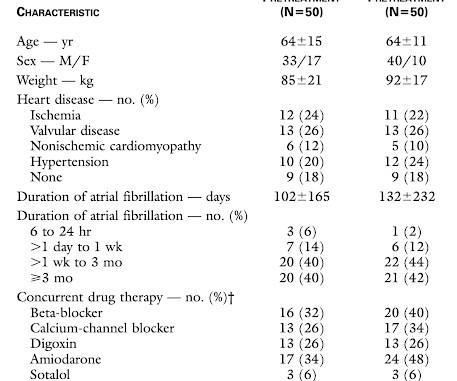
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. Methods. . =
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. That this might happen should not be surprising — since the patient's chest pain was already ongoing for 3 hours prior to arrival in the ED.
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. What does a heart look like on ultrasound when the EKG looks like that?
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. As per Dr. Smith — the intuitive answer should be obvious.
She was defibrillated and resuscitated. To Emphasize: The reason definitive diagnosis is important in today's case — is that the senior ED physician interpreted ECG #1 as "nothing too exciting". Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
On ED arrival ROSC is achieved. As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. They are unable to feel a pulse and resume CPR. The receiving staff suspects pulmonary embolism due to S1Q3T3 on the ECG and administers TPA.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chest pain that started 2-3 hours earlier while sitting on a porch swing. Here is her ED EKG: What do you think? She was successfully defibrillated and taken back to the ED. But which artery? The family sued.
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready. Resuscitative attempts were initiated quickly. Eventually asystole, and the patient died.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergency department (ED). His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. It is unclear how long he was down.
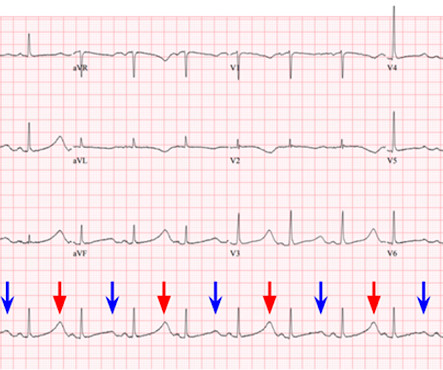
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Upon closer inspection, the defibrillator's monitor had assigned a spike for every large T wave as well as every QRS complex.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content