This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
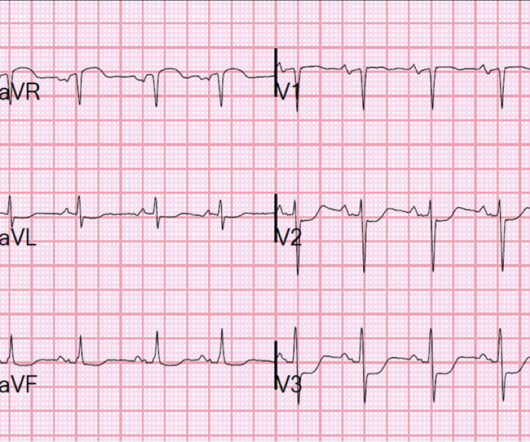
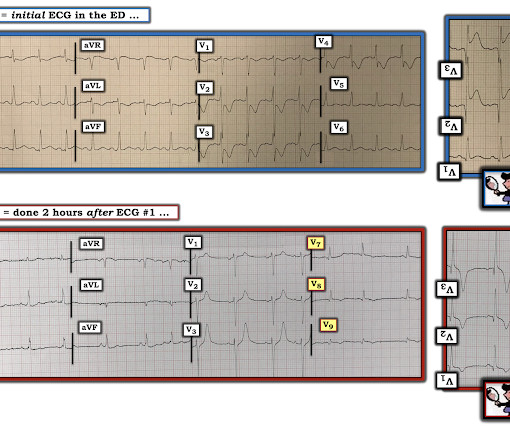
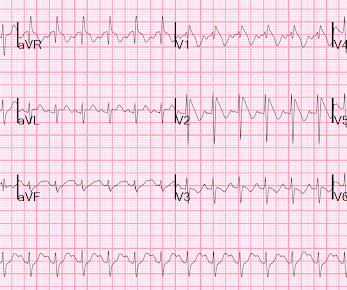
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. Lemkes JS, Janssens GN, van der Hoeven NW, et al.
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. Further information is not available.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. After 1 mg of epinephrine they achieved ROSC.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chest pain that started 2-3 hours earlier while sitting on a porch swing. Here is her ED EKG: What do you think? See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria).
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. A middle-aged male had a V Fib arrest. He had a history of CAD with CABG.
It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
This post will focus on the key parts of the guideline that affect ED evaluation and management. With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. Editorial Comment : Yes to PCI after arrest with STEMI on ECG.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? It is a STEMI equivalent.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. He appeared to be in shock.
RBBB in acute STEMI has a very high mortality. But here there is a large degree of ST elevation in V2-V6, I, and aVL. The paramedics activated the cath lab from the field.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. A healthy 45-year-old female presented with chest pain, with normal vitals.
So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Bedside echo revealed anteroseptal wall motion abnormality at which point I activated a code STEMI. Defibrillated out of v fib in the cath lab. mm in men over age 40.
Here is his ECG on presentation to the ED, approximately 45 minutes after onset of pain, but with pain improving since onset: What is your interpretation? The initial ECG was interpreted as "normal" by the computer ( Algorithm: Marquette GE / 12SL ) and "no acute ischemic changes" by the ED physician.
If it is STEMI, it would have to be RBBB with STEMI. Only 5-18% of ED patients with chest pain have a myocardial infarction of any kind. Cardioversion/defibrillation. The patient presented with chest pain. Here is the ECG: What do you think? I frankly did not know what to think. Is it Brugada pattern? Only 1-5% have OMI.
She was defibrillated and resuscitated. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. CPR was initiated immediately.
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. Treatment is by ICD ( implantable cardioverter defibrillator ).
--If she has fever, she should aggressively take acetaminophen and/or ibuprofen and, if not improving, will need to go to ED for further evaluation. --If If there are any syncopal or presyncopal events, she should be evaluated immediately in the ED. --All All 1st degree relatives should have 1 time EGG. And another finding.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. A 12-lead was recorded, showing "STEMI," but is unavailable. She was brought to the ED in a deep coma with GCS of 3, with vital signs, and an ECG was recorded: What do you think?
Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. In other words, millimeters really don't matter!
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Defibrillation was performed, and ROSC was achieved. Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it.
Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. Throughout this process, the patient had repeated VF and was defibrillated 8 times. It is almost certainly not acute.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content