This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services at Tacoma Community College. Case: During a busy emergencydepartment (ED) shift the paramedic phone rings.
Case: A 6-month-old boy presents to the emergencydepartment (ED) with three days of worsening cough, cold symptoms, and fever. Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base. Pediatric Crit Care Med.
A 67-year-old man presents to the emergencydepartment (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation?
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Traditional Advanced Cardiovascular Life Support (ACLS) medications, namely epinephrine, have been known to exacerbate coronary vasospasm. Click to enlarge.)
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. He arrived in the emergencydepartment hemodynamically stable. This young male had ventricular fibrillation during a triathlon. On his bib it stated that he had a congenital heart disorder. His initial ECG is shown here.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. Association between calcium administration and outcomes during adult cardiopulmonary resuscitation at the emergencydepartment.
JAMA 2018 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a physician assistant practicing in emergency medicine in the Seattle area and an adjunct faculty member with the Tacoma Community College paramedic program. Key to survival is high-quality CPR and early defibrillation.
The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization. The arrhythmia spontaneously converted before defibrillation was achieved. Just prior to arrival he fell out of consciousness with the below ECG on the monitor. ECG #3 The above ECG shows a polymorphic VT at a rate of about 180 BPM.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergencydepartment (ED). You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Am J Emerg Med. What would your next steps be? N Engl J Med.
With ventilations and epinephrine, she regained a pulse. She was never seen to be in ventricular fibrillation and was never defibrillated. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. A middle-age woman with h/o hypertension was found down by her husband.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. What do you think?
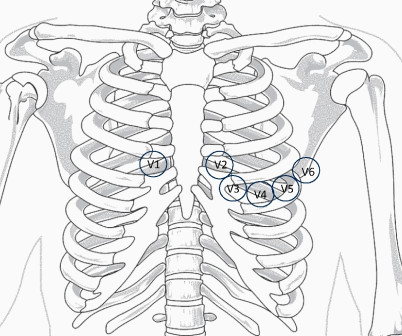
I B ECG monitoring should start immediately and a defibrillator must be ready. I B Patients transferred to PCI centres can bypass the emergencydepartment to undergo primary PCI without delay. STEMI , ST-segment elevation acute myocardial infarction ). due to reciprocal ST-segment depressions in V1, V2, V3).
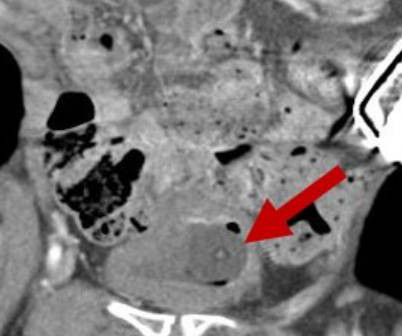
Holy Foley A Rare Case of Iatrogenic Obstruction by Adam Heilmann, MD; Jessica Pelletier, DO; Jennifer Reyes Lin, MD, MPH Our patient is a 33-year-old male with spastic quadriparesis due to cerebral palsy with chronic indwelling suprapubic catheter (SPC) who presented to the emergencydepartment (ED) due to concern for Foley catheter obstruction.
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. EmergencyDepartment Two-Dimensional Echocardiography in the Diagnosis of Nontraumatic Cardiac Rupture. A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. Plummer D et al.
In the standard care of anaphylactoid reactions, we administer Epinephrine, Diphenhydramine, steroids, and bronchodilators. Sure, we still do CPR, defibrillate as needed, and give Epinephrine based upon our local guidance. Could this work for the AFE patient? The American Academy of Obstetrics and Gynecology isn’t sure.
He was defibrillated twice and received two doses of epinephrine, with return of spontaneous circulation. Initial echocardiogram (ECG) on arrival (see figure 2) to our emergencydepartment revealed normal sinus rhythm, mild interventricular conduction delay (RSR’), and possible right ventricular hypertrophy.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content