This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: January 11, 2024 Guest Skeptic: Dr. Chris Root is an EMS fellow in the Department of Emergency Medicine at the University of New Mexico Health […] The post SGEM#426: All the Small Things – Small Bag Ventilation Masks in Out of Hospital Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Resuscitation 2023.
The post Ep 169 Cardiac Arrest Controversies – Chest Compressions, Dual Defibrillation, Medications and Airway appeared first on Emergency Medicine Cases.
In anticipation of EM Cases Episode 112 on Tachydysrhthmias with Amal Mattu and Paul Dorion, Melanie Baimel tells her Best Case Ever of a previously healthy young man who presents in refractory ventricular fibrillation after receiving multiple single shocks, ongoing chest compressions, several rounds of epinephrine, amiodarone and dual sequence defibrillation (..)
A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). Date: December 6th , 2018 Reference: Perkins et al.
After administering 1mg of epinephrine ROSC is noted with a bradycardic rhythm ( Figure 2 ). As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. Junctional Rhythm, occasional PAC's, and artifact.
Case: You are the Chief of your local Fire and EMS Department, and an individual contacts you saying […] The post SGEM#380: OHCAs Happen and You’re Head Over Heels – Head Elevated During CPR? Head and thorax elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC? first appeared on The Skeptics Guide to Emergency Medicine.
Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado. Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado.
EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% They started CPR.
Case: You are the medical director of an EMS system in a large city deciding on whether to respond to all out of hospital cardiac arrests (OHCA) with ACLS capabilities, or if resources should be directed to those candidates for extracorporeal CPR. You need to recognize an arrest and activate your EMS system. vs. 66.8%, p=0.73).
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
Case: EMS arrive to your emergency department with a 68-year-old man post cardiac arrest patient. Key to survival is high-quality CPR and early defibrillation. They had a difficult time getting a definitive airway pre-hospital. It required multiple attempts which caused several prolonged interruptions in CPR. What should you tell him?
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University in St. Louis); Dr. Jessica Pelletier, DO (EM Attending Physician, Washington University in St. You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Per EMS he was very cold to touch.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. Epinephrine infusion was begun. He required multiple defibrillations within a period of a few hours. An ICD ( Implantable Cardioverter Defibrilator ) was placed prior to discharge.
For all the fancy changes over the year, the bottom line has always been to provide good CPR compressions and timely defibrillation. The pediatric epinephrine and norepinephrine infusion rates have been lowered to 0.1-0.5 The pediatric epinephrine and norepinephrine infusion rates have been lowered to 0.1-0.5 mg via syringe.*
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Population: Patients > 18 years of age w/ OHCA treated by 10 EMS systems in in the US. Head Up (HUP) CPR may be the next critical improvement.
Alongside tracheal intubation , response times , and fire-based EMS, this is one of the most controversial topics in prehospital medicine. This is important because too many EMS systems look at mechanical CPR as a way to avoid having to become experts in resuscitation or having to send additional resources to the scene.
EMS arrived and found her in a wide complex PEA rhythm. She was given 3 mg IV epinephrine and multiple rounds of ACLS over approximately 20 minutes. She was never defibrillated. This is commonly found after epinephrine for cardiac arrest, but could have been pre-existing and a possible contributing factor to cardiac arrest.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. His family has been performing bystander, and report that he suddenly collapsed just a few minutes ago.
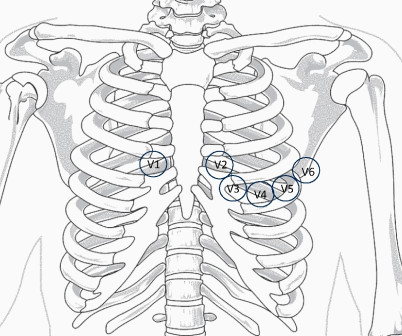
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). On epinephrine and norepinephrine drips."
EMS physicians report he was found in ventricular fibrillation. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation? He was found by bystanders after he collapsed and 911 was called.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Chest compressions were continued, and the patient was given 1 round of epinephrine, calcium, bicarb, glucose.
EMS found the patient pulseless and apneic, with an initial rhythm showing ventricular fibrillation. He was defibrillated twice and received 2 doses of epinephrine, with return of spontaneous circulation. There was no family history of syncope or sudden death. Click here for the full article!
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Annals of EM 23(6):1333-1342; June 1994. A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. She collapsed and 911 was called; she was found pulseless. Exact rhythm during arrest is uncertain.
Resuscitated with chest compressions, epinephrine. including epinephrine, and there was ROSC. Smith makes the key point that had this arrest witnessed by the medic team been the result of an acute cardiac event ( therefore, presumably VT or VFib ) prompt defibrillation by on-the-scene medics would most probably have resuscitated her.
Earlier in the summer, I wrote a blog discussing the challenges, intricacies, and educational pitfalls of postpartum hemorrhage in EMS. In the standard care of anaphylactoid reactions, we administer Epinephrine, Diphenhydramine, steroids, and bronchodilators. I even know of cases that my colleagues have managed!
EMS found the patient pulseless and apneic, with an initial rhythm showing ventricular fibrillation (see figure 1). He was defibrillated twice and received two doses of epinephrine, with return of spontaneous circulation. Figure 1: The EMS rhythm strip. There was no family history of syncope or sudden death.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content