This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: January 11, 2024 Guest Skeptic: Dr. Chris Root is an EMS fellow in the Department of Emergency Medicine at the University of New Mexico Health […] The post SGEM#426: All the Small Things – Small Bag Ventilation Masks in Out of Hospital Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Resuscitation 2023.
She is also the local director of the difficult airway EMS course at Washington State. Case: EMS arrives with a 58-year-old woman who suffered an out-of-hospital cardiac arrest (OOHCA). Despite that weak evidence, placement of IO in OOHCA has become a routine procedure for many EMS providers. Prehospital Emergency Care.
NEJM 2023 Guest Skeptic: Dr. Jeff Jarvis is the Chief Medical Officer and System Medical Director for the Metropolitan Area EMS Authority in Fort Worth, Texas, also known as MedStar. Jeff Jarvis is the Chief Medical Officer and System Medical Director for the Metropolitan Area EMS Authority in Fort Worth, Texas, also known as MedStar.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
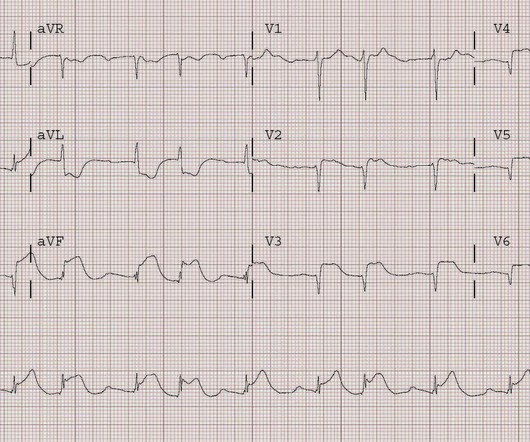
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration.
His roommate found an empty pill bottle on the floor next to him. The bottle contained 100 mg quetiapine tablets, and 50 tablets were unaccounted for. Second-generation antipsychotics (see Table 1 below) improve both positive and negative symptoms of schizophrenia and are less likely to be associated with EPS.
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC? first appeared on The Skeptics Guide to Emergency Medicine.
As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. Learning points: TCP is primarily recommended for bradycardia that does not respond to atropine, or other agents. It cannot be emphasized enough: You must be very skeptical of TCP.
Case: You are the Chief of your local Fire and EMS Department, and an individual contacts you saying […] The post SGEM#380: OHCAs Happen and You’re Head Over Heels – Head Elevated During CPR? Head and thorax elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival.
You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive.
Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado. Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado.
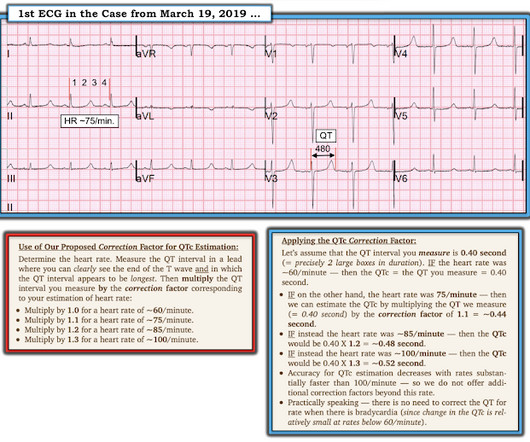
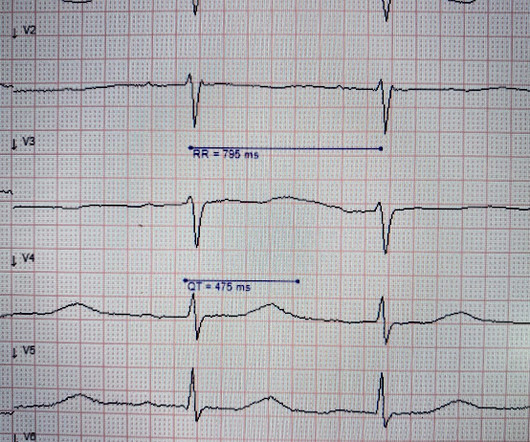
Dodd KW, Elm KD, Dodd EM, Smith SW. T-waves are quite tall and possibly peaked (HyperK?), but potassium returned normal. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis. What is the QT interval? Bogossian et al. (1) 2014;11:22732277.
We’ll keep it short, while you keep that EM brain sharp. A 36-year-old female presents to the ED after experiencing an episode of sudden syncope. The patient has no significant past medical history, and reports that she was walking to the end of her driveway to retrieve her mail when she suddenly collapsed to the ground.
EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. This patient was witnessed by bystanders to collapse.
He is a former New York City paramedic and this summer will be starting fellowship training in EMS medicine at UNM. A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Reference: Smida et al.
After reviewing over 12 million EMS incidents that took place in 2023 , the 2024 ESO EMS Index highlights two critical areas that demand attention: Early CPR and Opioid Use Disorder (OUD). Bystander CPR has been shown to double survival rates compared to cases where no CPR is performed prior to EMS arrival. Want to learn more?
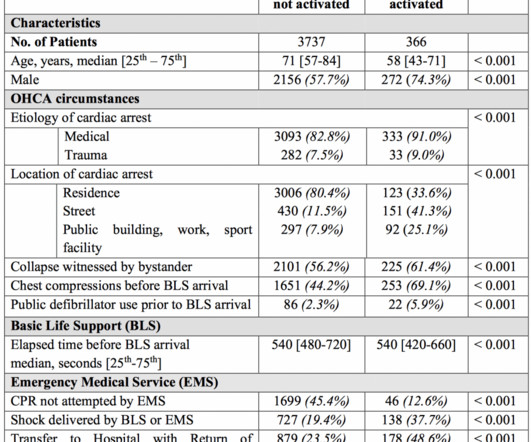
Case: You are the medical director of an EMS system in a large city deciding on whether to respond to all out of hospital cardiac arrests (OHCA) with ACLS capabilities, or if resources should be directed to those candidates for extracorporeal CPR. You need to recognize an arrest and activate your EMS system.
You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. Case: A 51-year-old man experiences a cardiac arrest on the street. He is unsuccessfully shocked.
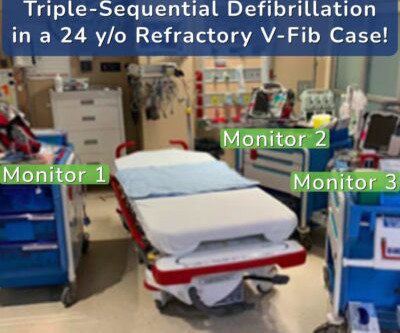
A recent case has highlighted the extraordinary potential of a novel intervention: triple-sequential defibrillation. The Case Unfolds Despite 82 minutes of high-quality CPR and Advanced Cardiovascular Life Support (ACLS) management, standard and dual-sequential defibrillation failed to restore the patient’s heartbeat.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR. Here is the initial ED ECG.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
In the realm of emergency healthcare, the terms EMS (Emergency Medical Services) and EMT (Emergency Medical Technician) are often used interchangeably, yet they represent distinct aspects of medical response and care. Though they are closely related and often work together, EMS and EMT have distinct roles, training, and responsibilities.
Case: EMS arrive to your emergency department with a 68-year-old man post cardiac arrest patient. Key to survival is high-quality CPR and early defibrillation. They had a difficult time getting a definitive airway pre-hospital. It required multiple attempts which caused several prolonged interruptions in CPR.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University in St. Louis); Dr. Jessica Pelletier, DO (EM Attending Physician, Washington University in St. You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Per EMS he was very cold to touch.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation.
Known cardiac defibrillator. appeared first on REBEL EM - Emergency Medicine Blog. Design: Prospective, observational, before and after implementation of a protocol study. Excluded: Obvious cause for OHCA prior to SDCT or on hospital arrival. Known obstructive coronary artery disease or known coronary stent. Pre-existing DNR order.
SGEM#64 : Classic EM Papers (OPALS Study) * SGEM#136 : CPR – Man or Machine? Cardiac Arrest: Pulselessness requiring chest compressions and/or defibrillation, with a hospital wide or unit based emergency response. He is currently deployed, practicing emergency medicine in an undisclosed location.
Fire/EMS crews found him clammy and uncomfortable. Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. Breath sounds were clear in all lung fields. No appreciable skin pallor.
A 56 yo f with h/o HTN and hypercholesterolemia called EMS from home after onset of L chest pain radiating to the left arm. Before EMS arrived, she had "seizure activity" and became unresponsive. She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. She was intubated.
Today we’re taking a more serious look at language, this time highlighting the terminology used by members of the Emergency Medical Service (EMS) community. The post Most EMS Terminology Comes Down to Initials, Abbreviations and Acronyms appeared first on National Center for Outdoor & Adventure Education.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chest pain. Upon EMS arrival the patient appeared acutely ill and complained of chest pain. An ECG was recorded immediately and is shown below. The patient is unstable.
Authors: Adam Roussas, MD, MBA, MSE // Reviewed by: Jamie Santistevan, MD ( @jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD ( @MPrizzleER ); and Brit Long, MD ( @long_brit ) Case A 40-year-old female presents to the emergency department for palpitations and lightheadedness. She denies chest pain.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiac arrest with return of spontaneous circulation. She was successfully revived after several rounds of ACLS including defibrillation and amiodarone.
Her husband called EMS when the patient experienced new onset seizures accompanied by micturition. The ECG below was recorded by EMS. This episode self terminated before defibrillation was possible. Written by Magnus Nossen — with edits by Grauer. The patient in today’s case is a 30-something female. What is your assessment?
In Basic Life Support (BLS) emergencies, a single EMS provider can not deliver optimum care, such as when trying to hold direct pressure on a bleeding wound, while preparing bandages, to stop bleeding. In Advanced Life support (ALS) emergencies, a “single” paramedic or ER doctor can not deliver necessary care.
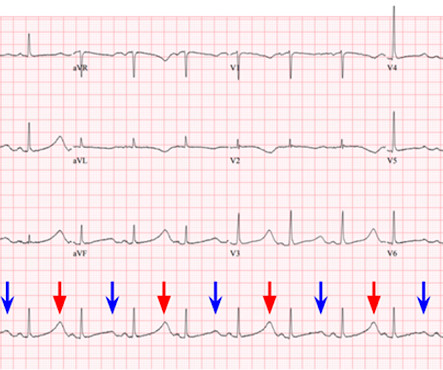
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. A 12 Lead ECG was recorded secondary to bizarre telemetry findings at bedside. Said differently, it’s a mess. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it.
They learn to operate sophisticated life-saving tools, from defibrillators to advanced airway management devices. My name is Mike, and I am thrilled to be able to share my extensive EMS experience with you. Climbing the Ladder A career as an EMT is a gateway to numerous opportunities within the medical field.
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Population: Patients > 18 years of age w/ OHCA treated by 10 EMS systems in in the US. Head Up (HUP) CPR may be the next critical improvement.
PMID: 34904190 Not surprisingly, this paper has been covered by basically everyone who talks about research, so if you want to hear some other opinions, check out the SGEM , REBEL EM , or St. PMID: 35490863 Hands on defibrillation: Even if it’s safe, would it actually help? 2018 Sep 11;362:k3843. doi: 10.1136/bmj.k3843.
EMS was activated and recorded the following ECG (scanned from a prehospital ECG, so the quality is not perfect): Notice the small Q wave in V1 followed by a very large R-wave, with a prolonged QRS. This patient is 38 years old with hyperlipidemia. He was at the gym when he had the onset of chest pain. There is a wide S-wave in V6.
Alongside tracheal intubation , response times , and fire-based EMS, this is one of the most controversial topics in prehospital medicine. This is important because too many EMS systems look at mechanical CPR as a way to avoid having to become experts in resuscitation or having to send additional resources to the scene.
For all the fancy changes over the year, the bottom line has always been to provide good CPR compressions and timely defibrillation. EMS may transport children with behavioral emergencies aged 4 to 18 directly to urgent crisis centers, provided they meet criteria and the service has sponsor hospital approval.* mg via syringe.*
Upon arrival, you quickly assess the situation and spring into action, working to save a man's life through CPR and defibrillation. This includes checking monitors, defibrillators, airway management equipment, and other essential tools for stabilizing and transporting critically ill patients. And the best part?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content