This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. Lemkes JS, Janssens GN, van der Hoeven NW, et al.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria).
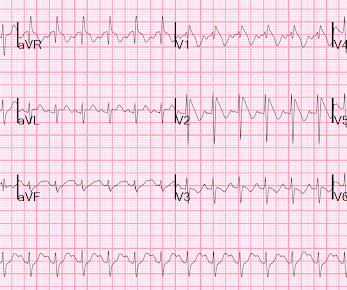
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B ECG monitoring should start immediately and a defibrillator must be ready.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome.
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. One must always be careful when looking for "baseline" ECGs, because the prior ECG on file may have been during another ACS event, as this one clearly was. This ECG is highly suspicious for LAD OMI.
Side note: contemporary troponin drawn 1 hour after acute LAD occlusion should usually be negative, unless the event has been going on longer than the patients symptoms. After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations.
She was defibrillated and resuscitated. Takotsubo is a sudden event, not one with crescendo angina. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. It is apparently fortunate that she had a cardiac arrest; otherwise, her ECG would have been ignored.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7].
Back to the case: After the patient was roomed, he revealed that he had undergone several episodes of syncope in the last 24 hours with each event resulting in a shock during which his wife reported that he would immediately awaken. The most recent event had occurred just before being triaged.
If there are any syncopal or presyncopal events, she should be evaluated immediately in the ED. --All This article is on Brugada in general, not just fever-induced: A score model to predict risk of events in patients with Brugada Syndrome Here is full text: [link] This was a single center cohort of 400 patients with Brugada syndrome.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. A 12-lead was recorded, showing "STEMI," but is unavailable. PEA is uncommon as an initial rhythm witnessed by EMS on the scene when the cause is an acute ischemic event.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Defibrillation was performed, and ROSC was achieved. Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it.
Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. Throughout this process, the patient had repeated VF and was defibrillated 8 times. It is almost certainly not acute.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content