This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Further information is not available. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.
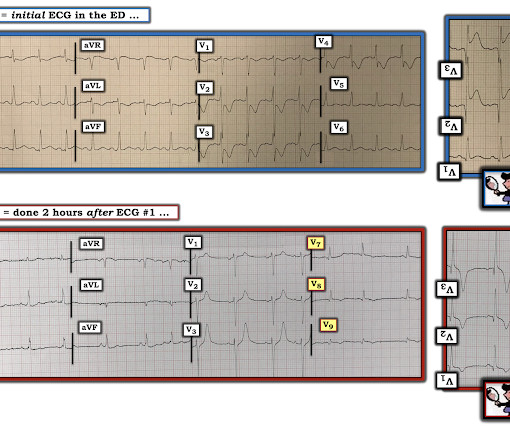
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI".
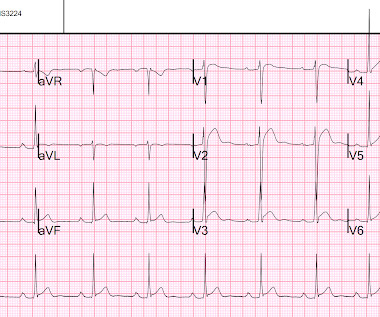
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The below ECG was recorded. What do you think?
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. This young male had ventricular fibrillation during a triathlon.
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. Remember that the ECG reports what is happening to the myocytes , then you must use that information to make inferences about what the patient needs. This ECG is highly suspicious for LAD OMI.
I sent this ECG with no clinical information to Dr. Smith. After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. A repeat ECG was done: Obvious anterolateral wall STEMI. It should have been shocked at least 10 seconds ago.
She was defibrillated and resuscitated. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
After reviewing the available information, cardiology did not feel that the patient warranted emergent PCI and recommended heparin infusion and cardiac catheterization the following morning. When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I CPR was initiated immediately.
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. For more information, see chapter 28 of Smith's " The ECG in Acute MI." Plummer D et al.
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. Treatment is by ICD ( implantable cardioverter defibrillator ).
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content