This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
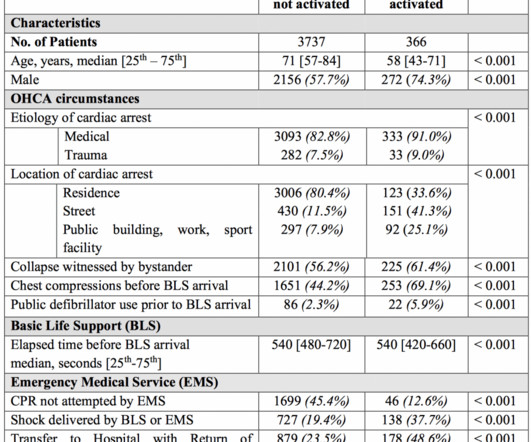
On your arrival, first responders from the fire department are performing high-quality basic cardiac lifesupport. You continue with compressions and defibrillations and your partner places an advanced airway. The patient is a 54-year-old man who collapsed in front of his family after complaining of chest pain for several hours.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
Prehospital advanced cardiac lifesupport for out-of-hospital cardiac arrest: a cohort study. He is also the CME editor for Academic Emergency Medicine and the associate editor for emergency medicine simulation at the […] The post SGEM#189: Bring Me To Life in OHCA first appeared on The Skeptics Guide to Emergency Medicine.
A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. This was a before and after study to see if advanced cardiac lifesupport (ACLS) techniques, including IV epinephrine, would improve survival to discharge. Case: A 51-year-old man experiences a cardiac arrest on the street.
You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive. SGEM#64 : Classic EM Papers (OPALS Study) * SGEM#136 : CPR – Man or Machine?
EMS arrives on scene and initiates high quality basic lifesupport (BLS). One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. We now know that an emphasis on the basics (high quality chest compressions and defibrillation) are the most important aspects of resuscitation.
A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Case: A paramedic crew responds to a 54-year-old male in cardiac arrest at a private residence. Reference: Smida et al.
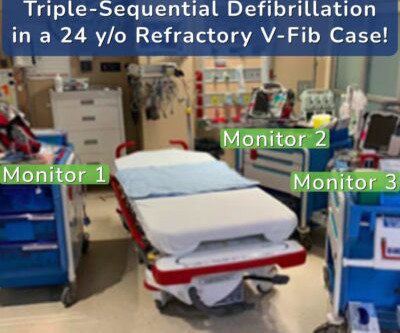
A recent case has highlighted the extraordinary potential of a novel intervention: triple-sequential defibrillation. This groundbreaking technique was used to save the life of a 24-year-old male who experienced an out-of-hospital cardiac arrest with refractory ventricular fibrillation. does not make clinical or medical decisions.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac lifesupport (ALCS), and Intubation. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Many of these OHCAs are due to ventricular fibrillation or pulseless VT.
The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field. The patient is moved over to the stretcher and connected to the monitors and defibrillator. What would your next steps be? His point-of-care labs return with a potassium of 3.4
With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. Consider administering epinephrine after defibrillation in those with shockable rhythms. COR 2b, LOE B-R. COR 2b, LOE B-R. COR 3, No benefit, LOE B-R. COR 2a, LOE B-NR.
Advanced cardiac lifesupport protocol was initiated, and the patient was intubated. After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Click to enlarge.)
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal lifesupport). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion.
This could range from basic lifesupport, typically managed by EMTs, to more advanced lifesupport provided by paramedics and other medical specialists. This equipment ranges from basic first aid supplies to sophisticated devices like defibrillators, oxygen therapy units, and advanced airway management tools.
In Basic LifeSupport (BLS) emergencies, a single EMS provider can not deliver optimum care, such as when trying to hold direct pressure on a bleeding wound, while preparing bandages, to stop bleeding. In Advanced Lifesupport (ALS) emergencies, a “single” paramedic or ER doctor can not deliver necessary care.
Cardiac arrest was called and advanced lifesupport was undertaken for this patient. She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. After about 90 seconds of chest compressions she awoke.
That’s because one of our areas of focus here at The National Center for Outdoor & Adventure Education (NCOAE) is emergency medicine training and education. The post Most EMS Terminology Comes Down to Initials, Abbreviations and Acronyms appeared first on National Center for Outdoor & Adventure Education.
I recerted CPR, ACLS (Advanced Cardiac LifeSupport) and PALS (Pediatric Advanced LifeSupport) late in December. For all the fancy changes over the year, the bottom line has always been to provide good CPR compressions and timely defibrillation. Pediatric defibrillation doses should be 2j/kg, 4j/kg.
As EMTs, we’re always prepared to address these life-threatening complications alongside the burns. Rapid Assessment and Advanced LifeSupport Upon arrival at the scene, our immediate focus is on assessing the victim’s airway, breathing, and circulation. Treating shock by keeping the victim warm and lying down.
More specifically, you have three fundamental job responsibilities: Assessment and stabilization of the patient’s condition Basic lifesupport Transportation In this post, we bring you up to speed on the different levels in emergency medicine and credentialing while explaining the basic education and skills required to become an EMT.
Similarly, funds can help purchase new defibrillators for paramedics, ensuring they have access to reliable equipment during critical life-saving moments. This training can include specialized instruction in areas such as hazardous material handling, advanced cardiac lifesupport, and technical rescue operations.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. His family has been performing bystander, and report that he suddenly collapsed just a few minutes ago. mEq/L (OR: 51.11; 95% CI: 3.12−1639.16;
The patient was put on Extracorporeal LifeSupport in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° In all leads, there is a 2nd wave after the initial QRS.
Besides going over the basic lifesaving skill of Cardiopulmonary Resuscitation, or CPR, you will learn the legal side of medicine, such as HIPAA, and emergencies that bring not only the end, but a new start, to life. Being Nationally Registered requires over 190 hours of coursework, which is equivalent to two college classes.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
<1% of patients present with high-grade parasitemia and life-threatening symptoms including myocarditis, pericardial effusion, meningoencephalitis, neuritis, or a combination of these. . Designated a neglected tropical disease by the WHO since 2005, CD remains under-diagnosed with a global case detection rate less than 10%.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content