This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (Ret) @DidlakeDW Expert contribution by Dr Robert Herman @RobertHermanMD @PowerfulMedical (Chief Medical Officer) An adult male called 911 for new-onset epigastric burning. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). She has a history of hypertension and non-insulin dependent diabetes mellitus.
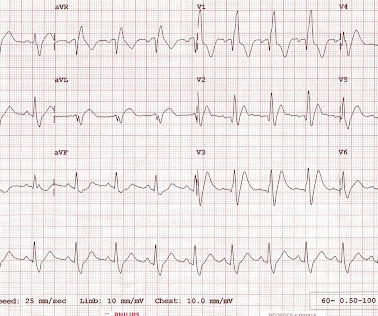
Written by Jesse McLaren Two 70 year olds had acute chest pain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. Who needs the cath lab?
RBBB in acute STEMI has a very high mortality. The paramedics activated the cath lab from the field. But here there is a large degree of ST elevation in V2-V6, I, and aVL.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. She was defibrillated and resuscitated. Learning Points: 1. From Gue at al.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, when someone has immediate resuscitation of an arrest witnessed by paramedics, they rarely have a GCS of 3 (deep coma).
The paramedics diagnosis was "Possible Anterolateral STEMI." We rapidly defibrillated her, and with return of normal sinus rhythm. Several minutes later the patient developed V-fib again > 200J defibrillation with return to NSR. More proof that a huge STEMI may have normal or near normal initial troponin.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content