This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
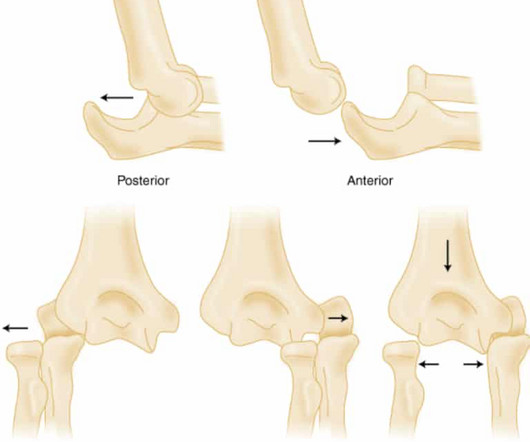
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
typhi infection if treatment is refractory to supportive measures or conventional community-acquired pneumonia antibiotics Treat with atypical bacterial coverage (doxycycline, azithromycin, chloramphenicol, or fluoroquinolones) A 32-year-old woman presents to the ED with a fever and rash after returning from a trip to Southeast Asia. .:
Definition: SBP is an infection of the peritoneal ascitic fluid without an intra-abdominal focus of infection. Commonly a monomicrobial infection with gram-negative bacteria like E. Paracentesis is a safe procedure with a low complication rate (< 1%). coli (50-90% of cases). increase in mortality.
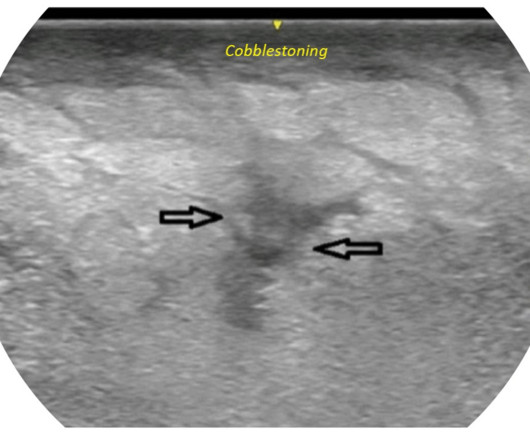
The definitive treatment of a necrotizing soft tissue infection is surgical debridement and removal of the necrotic tissue. REFERENCES: Castleberg E, Jenson N, Dinh VA. 2014;15(1):111-113. 2020;12(1). Accessed March 9, 2022. This is a tricky diagnosis that can often be inconspicuous, so clinical gestalt is key.
Since tonsillectomy is one of the most common pediatric surgeries in the US (~500,000 per year) and the rate of post-tonsillectomy hemorrhage is about 1-5% , it is a good idea that we all are familiar with how to manage this issue! Get a hold of ENT early as OR management and/or admission are common. Set up suction x2 in the room!
Definition A series of hemodynamic changes related to autonomic denervation and loss of sympathetic tone. Negative E-FAST and no signs of long bone injuries should raise concern for neurogenic shock in the hypotensive trauma patient with suspected spinal injury. Alpha 1 agonists are necessary to maintain appropriate blood pressure.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think?
Written By: Kaitlynn Tracy, MD Edited By: Sean Schnarr, MD and Gregg Chesney, MD Definition/Background: Burns are classified as being major, moderate, or minor in severity. 4 Survival rate for all burn injuries is around 97%, which is a notable increase from 75% in the 1960’s.
mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
to 1 case per 100,000 children. to 1 case per 100,000 children. 2][3] Definitive diagnosis is made by laryngoscopy or bronchoscopy showing normal or mildly erythematous epiglottis and an erythematous, edematous trachea with thick mucopurulent exudates. [3] 2] Bacterial infection usually preceded by viral infection.
It should be no surprise that academic clinical educators are at high risk for burnout, stalled career advancement, and abandonment of academic medicine altogether [1, 2]. Let’s start with the obligatory definition of coaching. She likes teaching, but are not sure residency or medical student education leadership is for her.
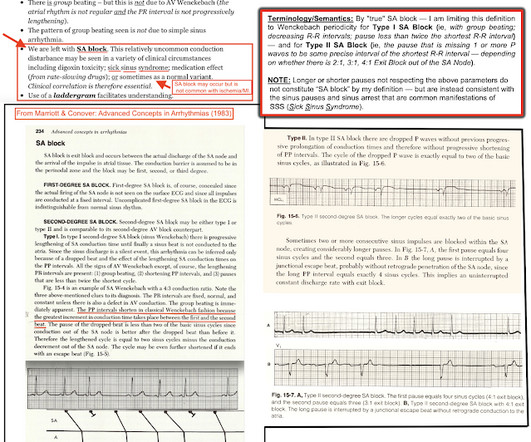
R waves 6 through 9 have no preceding P waves and are suspiciously regularly spaced. Impulses E, F, G, H, and I were blocked. Progress in Biophysics and Molecular Biology , 120 (1–3), 164–178. Science Translational Medicine , 9 (400). Janssen, P. & Fedorov, V. link] Li, N., Hansen, B. Ignozzi, A. Zakharkin, S.
1, 2 Its occurrence often portends worse outcomes in intubated patients, whose projected hospital course was already tenuous. 1, 4, 6 The overall incidence of VAP is somewhere around 5%-40% of all intubated patients, depending on the study and country from which it is reported. 4, 8 Paper: Dahyot-Fizelier, C.,
He has already climbed Ben Nevis in Scotland, visited the Gobi desert (possibly from the comfort of his parents 4 x 4, but who’s judging) and has his bronze D of E nailed. She calls out her findings: A – OK B – 1 puncture mark to the anterior left chest wall, covered with a three-sided dressing. RR 25-30. Actively oozing.
Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). Answer : Bedside ultrasound!
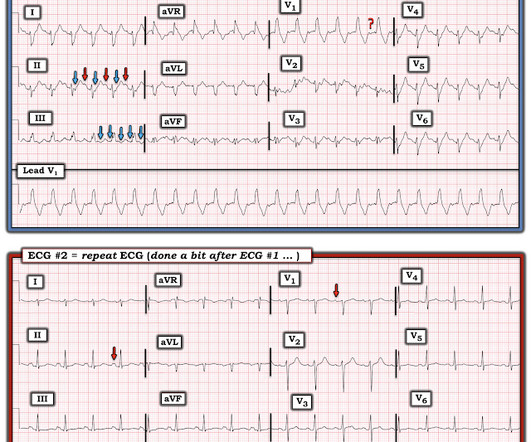
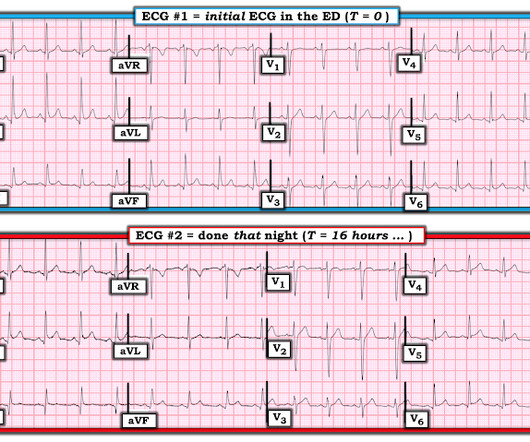
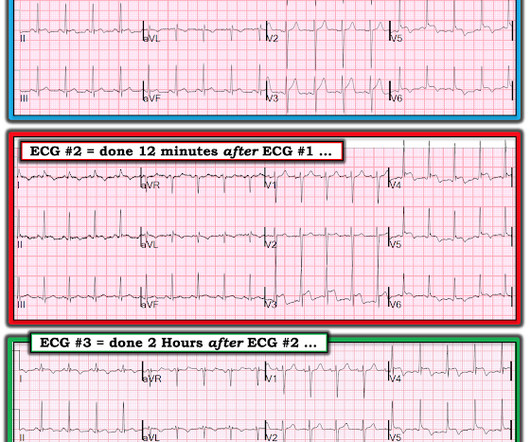
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1? —
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
1 Risk Factors: 1-4 Spontaneous Anticoagulants (Apixaban, Rivaroxaban, etc.) Older Age (median age of 70 years) 1 Abnormal vasculature/neoplasm of the kidney (e.g., 5 Clinical Presentation: 1-3 Variable presentation but may present with dropping hemoglobin/hematocrit without other findings in spontaneous cases.
REBEL Core Cast 107.0 – Vertebral Osteomyelitis Click here for Direct Download of the Podcast Definition Inflammation of the vertebrae due to a pyogenic, fungal or mycobacterial organism. Epidemiology 1 to 2.4 Epidemiology 1 to 2.4 Other pathogens include: E. Often used interchangeably with osteomyelitis.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% He denied chest pain or shortness of breath.
Historically, the endotracheal tube (ETT) has been considered the definitive airway of choice in both the prehospital and in-hospital setting. 1 Prehospital endotracheal intubation and EGAs are typically placed without paralytics and are reserved for unconscious, apneic, and out-of-hospital cardiac arrest patients.
Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ). Figure-1: Comparison between the first 3 ECGs in today's case. How Would YOU Interpret the Serial Tracings in Figure-1? No wall motion abnormality identified.
On examination, she has erythema and tenderness overlying her left parotid gland. Massaging the gland causes expression of purulent material. What is the diagnosis?
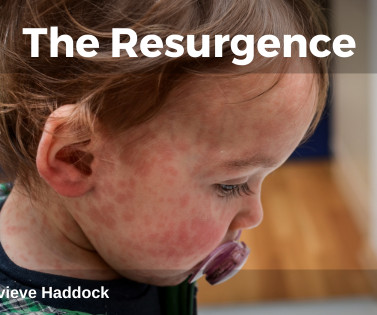
Coverage of the 6-in-1 vaccine measured at 12 months of age in England for Q4 2023 to 2024 Source: ONS under the Open Government License v3.0 Young infants and immunosuppressed individuals are particularly at risk of severe disease, resulting in significant morbidity and associated mortality rates of 1-3 per 1,000 cases.
Question 1: What is the rhythm? They are not premature, by definition. Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. Said differently, it’s a mess. slowing of the heart rate).
Comprehensive physical exam is unremarkable, but she does have pain at the T-12/L-1 region of her back. Her patellar reflexes are 1+ bilaterally, no ankle clonus is noted, and she denies any saddle anesthesia or bowel/bladder incontinence. CT of lower spine is ordered and shows the following: 1 What is the diagnosis?
The lack of consistent definitions in the literature makes it difficult to report its true prevalence and hampers efforts to combat it. Here are ten things to think about: 1. Churruca K, Pavithra A, McMullan R, Urwin R, Tippett S, Cunningham N, Loh E, Westbrook J. cognitive rehearsal techniques ). Organizational dynamics.
1 While PJP gained significant recognition among HIV-positive adults during the early AIDS epidemic, the growing utilization of immunosuppressants has resulted in an increased incidence of the disease in individuals who are HIV-negative. 9 The signs and symptoms of PJP infection are non-specific. 0 C, and has no jaundice.
A point of care ultrasound of the liver reveals the following: Image 1: Ultrasound of the liver showing abnormal hepatic artery flow and resistance index 1 Question: What is the diagnosis? She came today because her sister is a nurse who noticed her eyes were yellow. She denies fever or a new rash. LFTs are in the thousands.
A biopsy is often ultimately required for a definitive diagnosis. You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? As clinicians, we need to be prepared.
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
A wide variety of conditions can result in either type of cholestasis (Figure 1). 1 Extrahepatic obstruction is due to mechanical obstruction occurring downstream of the hepatic ducts such as pancreatic disease, gallstone obstruction of the common bile duct, and cancer. 9 How are cholestatic labs defined?
Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED. The primary purpose of Table 1 is to provide a summary of baseline characteristics and demographics of the study population, presenting data in a clear and organized manner.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. Therefore, this does not meet the definition of myocardial infarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. But maybe not. Thelin et al.
We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. Atropine usually works in junctional rhythm with a narrow complex 9. What is the atrial activity? What to do?
It is commonly seen in the first couple of years of life and accounts for 1-5% of paediatric hospital admissions for those under two. Failure to thrive’ has many definitions We use standardized charts to document infant growth. E.g. cleft palat e. ‘failure to thrive’, describes a slow growth pattern.
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. QRS onset is the best location for ST segment comparison, and is the location recommended by Universal Definition of MI. He was treated with Ceftriaxone and azithromycin. He was admitted.
Article 1: Positive urine cultures without pyuria Wang ME, Jones VG, Kane M, et al. Article 1: Positive urine cultures without pyuria Wang ME, Jones VG, Kane M, et al. Clinical Course of Children 1 to 24 Months Old With Positive Urine Cultures Without Pyuria. 2024;24(1):111-118. Acad Pediatr. doi:10.1016/j.acap.2023.06.023
These are reasons why it does not look like OMI: 1. Definitive diagnosis is by MRI. Serial Troponins remained in the 9-11 range, w/o any large rise and/or fall, also atypical for OMI. Serial Troponins remained in the 9-11 range, w/o any large rise and/or fall, also atypical for OMI. flat ST segment in V4 2.
Over the last 1 week, her exertional chest pain became worse both in intensity and triggering threshold. She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. But the patient has active chest pain. link] Shvilkin et al.
It is unclear to me whether this case could represent 1) simple supply/demand mismatch due to increased demand from epinephrine, 2) Kounis syndrome (usually described as mast cell mediated coronary vasospasm during allergic reaction), 3) brief autolysed left main or LAD ACS with no findings on later echo and CT coronary angio, or 4) something else.
Add in PEFR <33% and SpO2 <92% Management of acute asthma* * as per BTS guidelines Acute asthma is managed in a stepwise fashion using the following guidelines. Intubation, however, can be a significant challenge in these patients.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. As you take another LOOK at ECG #1 — What is the relevance of the findings that I've labeled in Figure-1 ?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content