This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With emergency department (ED) volumes rising, administrators are eager to explore AI-driven solutions to improve patient safety and reduce staff burnout. They want to know how CHARTWatch integrates with electronic health records (EHRs), whether it can adapt to their patient ED population, and how clinicians respond to using the tool.
Written By: Kaitlynn Tracy, MD Edited By: Sean Schnarr, MD and Gregg Chesney, MD Definition/Background: Burns are classified as being major, moderate, or minor in severity. Br Med J (Clin Res Ed). EM Cases – Burn and Inhalation Injuries: Ed Wound Care, Resuscitation and Airway Management.” Tintinalli, et al. 295.6591.181.
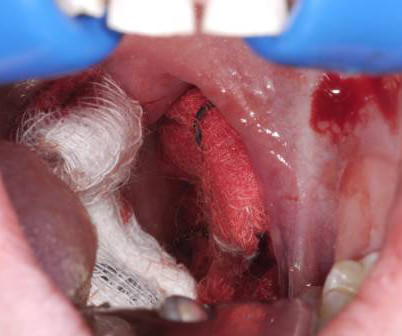
A young woman, 13 days post-tonsillectomy, comes into your rural emergency department (ED) coughing up blood. Managing post-tonsillectomy hemorrhage in the ED can be challenging, especially in rural or resource-limited settings. Hemoptysis ED approach and management. Its going to take time to get her to a tertiary center.
A 10-year-old boy presents to the emergency department (ED) after a high-speed motor vehicle collision. The study enrolled 22,430 children, aged 0–17 years, presenting with blunt trauma across 18 PECARN-affiliated ED in the US. Case Scenario: What would you do? He complains of neck pain and is reluctant to move his head.
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
He currently practices emergency medicine in New Mexico in the ED, in the field with EMS and with the UNM Lifeguard Air Emergency Services. Before attending medical school, he was a New York City Paramedic. Chris completed his emergency medicine residency and EMS fellowship at UNM.
One week prior to ED arrival, the patient was becoming progressively despondent, less interactive with peers, exhibiting slow speech and movements, and was not eating. In Diagnostic and statistical manual of mental disorders (5th ed.). Catatonia: a case report by Brown Emergency Medicine. Burrow JP, Spurling BC, Marwaha R.
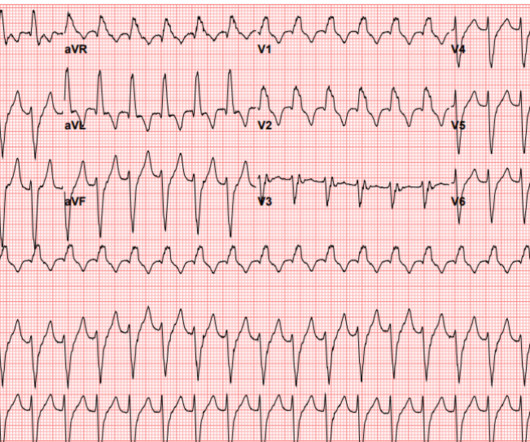
The Case A 41-year-old male presents to the ED with constant palpitations for one day. Differentiating between the two is difficult as multiple proposed diagnostic criteria have yet to demonstrate sufficient sensitivity or specificity for a definitive diagnosis. Discussion Fascicular VT is a distinct subgroup of idiopathic VT.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
Concussion – Presentation [ Silverberg, 2023 ] There is no definitive test to diagnose concussion in the ED. Mild traumatic brain injury also includes a larger group of injuries that may have evidence of structural injury.
These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED. Did they pick a heap of PEs?
A 52-year-old male with a history of essential hypertension presents to your South Texas ED for his second visit this week complaining of indolent fever, shortness of breath, pleuritic chest pain, and a rash on his trunk and extremities. We’ll keep it short, while you keep that EM brain sharp.
Definition A series of hemodynamic changes related to autonomic denervation and loss of sympathetic tone. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Main symptoms include hypotension and bradycardia. They may even need atropine and/or pacing for persistent bradycardia.
The ED clinician should inquire about a relevant history of HIV infection, malignancy, high-dose corticosteroid use, chemotherapy, organ transplant, or use of immunosuppressive drugs for other indications. She reports occasional central chest pain exacerbated by coughing. Int J STD AIDS. 2019;30(2):188-193. Am J Emerg Med. 2013;31(2):401-405.
Also known as Facilitated intubation (FI), the use of intubating with only a sedative was an accepted alternative intubation technique prior to those definitive studies in the late 1990s but quickly was abandoned for RSI in all emergent endotracheal intubations (ETI) (8,9). To date, ketamine has been the agent of choice (12).
Definition Transient LOC and loss of posture secondary to insufficient cerebral perfusion. Common – >25% lifetime incidence, 1% ED presentations … Continue reading →
Since the 2012 Berlin Definition of the Acute Respiratory Distress Syndrome (ARDS), several developments have supported the need for an expansion of the definition, including…
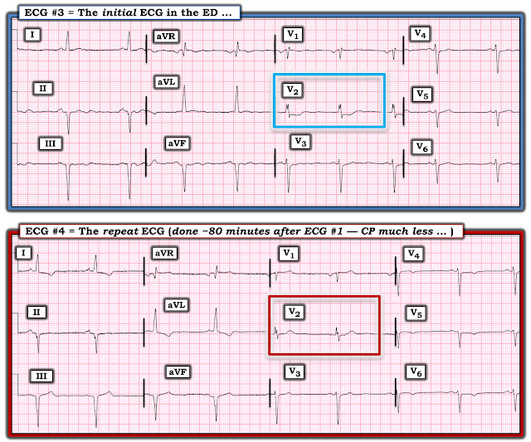
Figure-1: I've labeled the initial ECG in the ED. KEY Point: All patients who present to the ED for new CP should promptly have a triage ECG recorded, that is then immediately interpreted by the ED physician. For clarity — I've labeled this initial ECG in Figure-1.
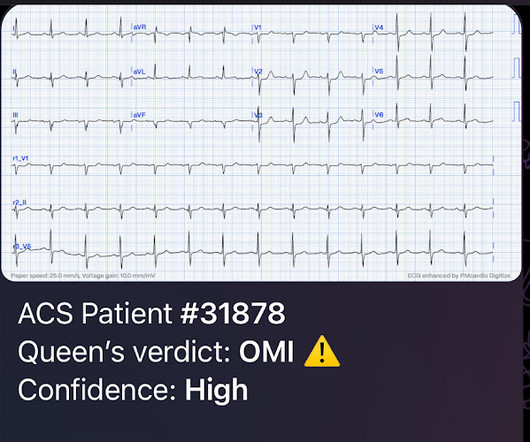
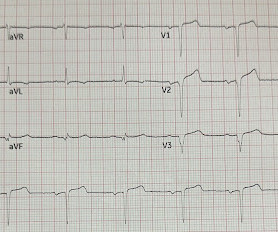
I simply texted back: "Definite posterior OMI." The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration.
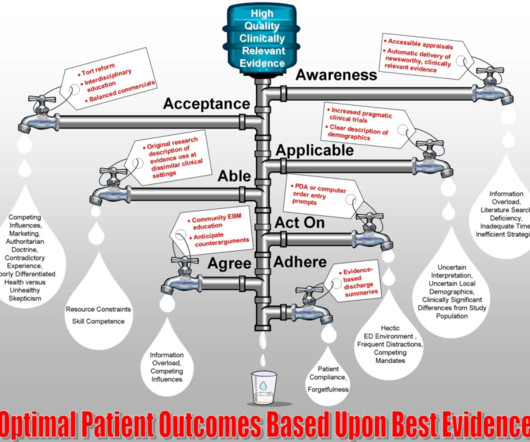
The bottom line from that episode on skin glue for peripheral intravenous lines was: “Skin glue does appear to decrease the failure rate of IVs in patients admitted to hospital from the ED at 48 hours. It was great that it started with a definition of evidence-based medicine (EBM).
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. Figure-1: I've labeled the initial EMS ECG and the 1st 12-lead tracing done on arrival in the ED.
1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. You will see that they were initially ischemic, by definition, because of the subsequent voltage attenuation. Chou’s Electrocardiography in Clinical Practice, 6th ed. second as the beginning of “wide”?
They've created a new protocol that allows them to bypass the ED and take qualified patients directly to definitive care. Teams in Arkansas are finding new ways to improve outcomes for pediatric behavioral health patients.
The DIMPLES study by PERUKI sought to investigate the incidence of new-onset diabetes in the paediatric population across the UK and Ireland, as well as the characteristics of these ED presentations, and to determine if SARS-CoV2 infection was involved. This meant 2746 ED presentations by 2618 individuals. Which patients were involved?
By some definitions, you could call former Maryland state legislator Dan Morhaim, MD, FACEP, a retired emergency physician. His health care focus included hospital efficiency, physician and patient satisfaction, and emergency department (ED) wait times, as well as a host of nonhealth issues. He thinks of it as re-deployed.
A 39-year-old male with history of achalasia with recent endoscopic dilation 24 hours prior presents to the ED for progressively worsening chest pain with radiation to his left shoulder. If there will be a delay in definitive management and there is evidence of intra-thoracic gastric contents, consider chest tube placement.
Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. These patients can be at risk of vomiting and aspiration and often prompts clinicians to pursue definitive airway management to avoid pneumonia and other complications.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
Here is his initial ED ECG: What do you think? Then the ED doc would be dependent on that first ECG. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) Or had not had a prehospital ECG on the ambulance.
9 Here are some of the key conditions that are considered neurodivergent and that emergency physicians are likely to encounter: Autism Spectrum Disorder (ASD): Although the definition of autism has changed over time, in general, it refers to a group of complex developmental brain disorders. How to assess children with complex needs in the ED.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2]
pneumatically), then definitively addressed by Orthopedics at their convenience. Traction splinting is usually not done in the ED. Ultrasound (eFAST) and plain x-rays (chest and pelvis) are useful tools for rapid evaluation in the ED. Orthopedic injuries should be manually reduced and perfusion ensured, splinted (e.g.
Here is the first prehospital ECG (time 0, after one hour of pain): I do not see evidence of OMI, and neither did the Queen of Hearts Here is the 2nd prehospital ECG (time 10 minutes, after 70 minutes of pain): No change On arrival, the first ED ECG was recorded 20 minutes after the last one (90 minutes after pain onset): What do you think?
2][3] Definitive diagnosis is made by laryngoscopy or bronchoscopy showing normal or mildly erythematous epiglottis and an erythematous, edematous trachea with thick mucopurulent exudates. [3] Labs and x-ray can be nonspecific, and definitive diagnosis is made with direct visualization. ampicillin-sulbactam).
Initial ED ECG: What do you think? Definitive diagnosis that ECG #1 is in fact VT is more than academic. That said — We can definitively diagnose AV dissociation in today's tracing! Once I knew that at least 1 definite underlying P wave was present — I diligently looked for more. Why did I say that?
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event.
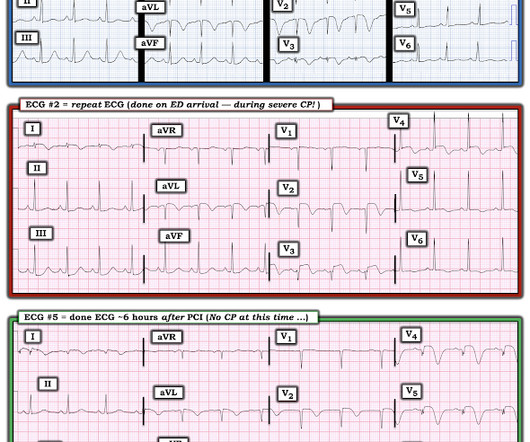
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" On arrival to the ED, while waiting for cath lab team, he obtained another ECG: You can now see the full voltage of the high-voltage QRS, likely with some degree of LVH. Both were awake and alert with normal vital signs.
Definition: SBP is an infection of the peritoneal ascitic fluid without an intra-abdominal focus of infection. Major takeaway: Consider SBP in any patient who comes into the ED with ascites. Primary spontaneous bacterial peritonitis (SBP) is one of the most common infections in those with cirrhosis and ascites.
An ED ECG, if recorded with pain, should show LAD OMI. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5. The Cath lab was activated.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content