This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case: The Chief of Emergency Medicine (EM) at a large urban hospital recently approached the AI Committee at Unity Health, intrigued by the CMAJ article describing the apparent success of CHARTWatch in detecting early signs of patient deterioration. Background: There are many ways to define artificial intelligence.
We’ll keep it short, while you keep that EM brain sharp. A 52-year-old male with a history of essential hypertension presents to your South Texas ED for his second visit this week complaining of indolent fever, shortness of breath, pleuritic chest pain, and a rash on his trunk and extremities. .: Infect Dis Rep.
Chris Root is an emergency medicine and emergency medicine service (EMS) physician at the University of New Mexico, Albuquerque. Chris completed his emergency medicine residency and EMS fellowship at UNM. Before attending medical school, he was a New York City Paramedic.
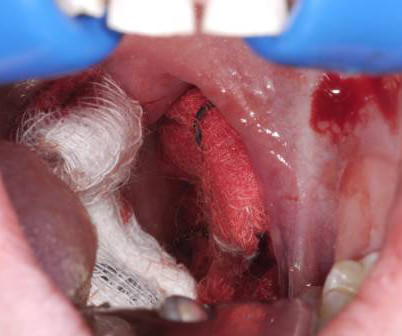
A young woman, 13 days post-tonsillectomy, comes into your rural emergency department (ED) coughing up blood. Managing post-tonsillectomy hemorrhage in the ED can be challenging, especially in rural or resource-limited settings. Hemoptysis ED approach and management. Its going to take time to get her to a tertiary center.
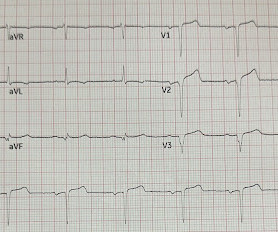
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians.
To get a sense of how medical students feel about emergency medicine, we interviewed three students who are interested in EM: Nick, a graduating M4 pre-matched into EM residency, Charlotte, an M2 currently planning to pursue EM, and Annie, an M1 considering EM. What sparked your interest in emergency medicine?
To get a sense of how medical students feel about emergency medicine, we interviewed three students who are interested in EM: Nick, a graduating M4 pre-matched into EM residency, Charlotte, an M2 currently planning to pursue EM, and Annie, an M1 considering EM. What sparked your interest in emergency medicine?
To celebrate the end of trauma season ( is it ever really over? ), we here at the Ped EM Morsels Bakery have cooked up a morsel to remind you that pediatric trauma can be even more difficult than you think. Definition A series of hemodynamic changes related to autonomic denervation and loss of sympathetic tone. Never fear.
Concussion – Presentation [ Silverberg, 2023 ] There is no definitive test to diagnose concussion in the ED. The post Return to Learn / Return to Sport after Concussion appeared first on Pediatric EM Morsels. Mild traumatic brain injury also includes a larger group of injuries that may have evidence of structural injury.
Definition Transient LOC and loss of posture secondary to insufficient cerebral perfusion. Common – >25% lifetime incidence, 1% ED presentations … Continue reading →
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Available from: [link] Guldner GT, Smith T, Magee EM.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with past medical history diabetes mellitus, hypertension, hyperlipidemia, dementia presents from nursing home with acute unilateral swelling along the left side of her face. On examination, she has erythema and tenderness overlying her left parotid gland.
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a history of poorly controlled diabetes presents to the ED with increasing right-sided ear and facial pain, swelling, and difficulty hearing for two weeks. He says the pain is worse at night and when he is chewing. What is the diagnosis?
We’ll keep it short, while you keep that EM brain sharp. A 41-year-old male with no significant past medical history presents with a deep hand laceration. The patient states they were cutting an avocado when the knife pierced through and punctured his hand. Rosh Review Website Link References: Park CW, Juliano ML, Woodhall D. In: StatPearls.
We’ll keep it short, while you keep that EM brain sharp. A 3-year-old male with no past medical history presents to the ED with one week of daily fevers >102°F associated with four days of rash on the trunk. In: Post TW, ed. In: Post TW, ed. In: Post TW, ed. In: Post TW, ed. C) for the past week.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think?
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
Authors: Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA), Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. Article: Hilsden R, Mitrou N, Hawel J, Leeper R, Thompson D, Myslik F. Discussion: Bias: In this study, selection bias had a significant impact.
Historically, the endotracheal tube (ETT) has been considered the definitive airway of choice in both the prehospital and in-hospital setting. Emergency medical services (EMS) scope of practice is governed by the state, but national scope of practice guidelines are available for the four different EMS provider levels.
1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. You will see that they were initially ischemic, by definition, because of the subsequent voltage attenuation. Chou’s Electrocardiography in Clinical Practice, 6th ed. second as the beginning of “wide”?
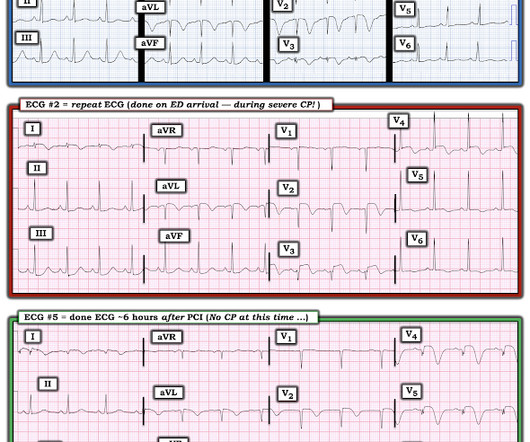
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. EMS arrived — and recorded 2 ECGs. The 3rd tracing in Figure-1 was the initial ED ECG — obtained at a time when the patient's CP had resolved. 14 minutes later — ECG #2 was recorded by EMS.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
EMS arrived and found him in Ventricular Fibrillation (VF). The patient was brought to the ED and had this ECG recorded: What do you think? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves.
We need high-quality evidence to provide a definite conclusion. Additionally, potential increases in resource utilization, healthcare expense, and ED length of stay are also essential considerations. However, there simply is not enough high-quality evidence to provide a definite conclusion.
An ED ECG, if recorded with pain, should show LAD OMI. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5. The Cath lab was activated.
Key Secondary Endpoints: 5 (3.9%) patients in the IV cetirizine group returned to any ED or clinic within 24 hours compared to 15 (11.1%) in the IV diphenhydramine group; P=0.04 7 (5.5%) patients in the IV cetirizine group returned to any ED or clinic within 48 hours compared to 19 (14.1%) in the IV diphenhydramine group; P=0.02
By Sofiya Diurba MD, reviewed by Meyers, Grauer A woman in her 50s with PMH known RBBB and prior syncopal events presents to the ED for five syncopal events over the last 24 hours. EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport.
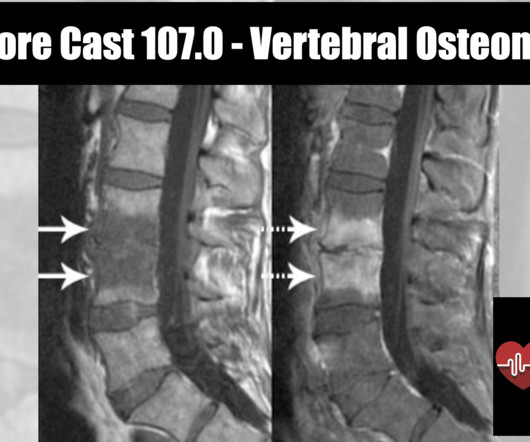
REBEL Core Cast 107.0 – Vertebral Osteomyelitis Click here for Direct Download of the Podcast Definition Inflammation of the vertebrae due to a pyogenic, fungal or mycobacterial organism. In: Sherman SC eds. Vertebral Osteomyelitis and Spinal Epidural Abscess: An Evidence-based Review. J Spinal Disord Tech. Semin Arthritis Rheum.
REBEL Core Cast 114.0 – Carbon Monoxide Toxicity [“[link] Click here for Direct Download of the Podcast Definition and Physiology Carbon monoxide is absorbed via inhalation from the incomplete combustion of any carbon containing substance. Ann Clin Lab Sci. 1976 Jul-Aug;6(4):372-6. PMID: 962299. Tomaszewski C. Chapter 122.
A 58-year-old male with a history of alcohol abuse presented to the emergency department (ED) as a category 2 trauma for a fall with a reported flail chest. EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest. J Surg Res.
If that sounds distinctly definitive, then point purposefully made. Factoring such, an order to transfer the patient immediately by ground or air EMS is the only actual support per se these non-physicians receive. Does this lack of balance I promote equate to no role(s) for non-physicians in an emergency department?
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine.
The risk of a biphasic reaction is what keeps patients in the ED while being observed for a set period of time. This varied incidence can be due to inconsistent definitions or inclusion of mild reactions. appeared first on REBEL EM - Emergency Medicine Blog. up to 23% ( Lieberman 2005 , Rohacek 2014 , Tole 2007 , Grunau 2014 ).
Johnson, MD ( Community EM, Salina Regional Health Center) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF); Marina Boushra, MD (Cleveland Clinic Foundation, EM-CCM); Brit Long, MD (@long_brit) Case A 40-year-old woman presents to a rural emergency department (ED) with left leg pain and swelling for the past 5 days.
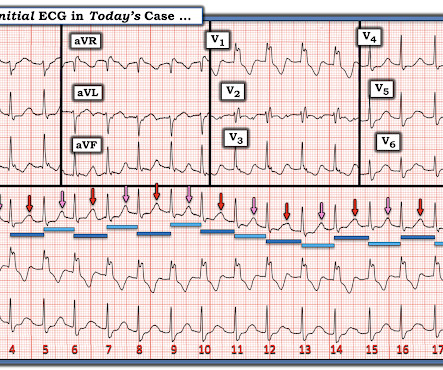
EMS was dispatched for a 30-something male who feels his heart is racing. Is it definitely VT?? He arrived in the ED and had an immediate bedside cardiac ultrasound while this ECG was being recorded. To illustrate this concept — I've reproduced in Figure-1 , the initial ECG recorded on today's patient in the ED.
On arrival in the ED, the patient denied any symptoms at all. No chest pain, no shortness of breath, no back pain, no numbness, weakness, tingling, no seizures or history of seizures, First ED ECG This still shows apparent inferior OMI. Figure-1: The initial ECG in today's case — obtained by the EMS team. (
The performance of EDs in 2020 and into 2021 changed abruptly, and that carried through into 2022. EDs weathered attacks from a variety of sources in recent years. ED leaders worked to develop new physician documentation and coding guidelines that needed to be implemented at the beginning of 2023.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. After all, there is no S wave in lead V3.
This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. The impact of push-dose phenylephrine use on subsequent preload expansion in the ED setting. 2015;10(3):e0119331. PMID: 25789927 Schwartz MB, et al. Am J Emerg Med. Am J Emerg Med.
When EMS found her, she was dyspneic and diaphoretic. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). She was out walking her dog when she developed sudden dizziness and light-headedness.
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED.
A biopsy is often ultimately required for a definitive diagnosis. You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? Arch Dis Child Educ Pract Ed. J Thorac Oncol.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiac arrest with return of spontaneous circulation. On arrival to the ED the patient was intubated with normal vital signs. No ischemic ST changes.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content