This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With emergency department (ED) volumes rising, administrators are eager to explore AI-driven solutions to improve patient safety and reduce staff burnout. They want to know how CHARTWatch integrates with electronic health records (EHRs), whether it can adapt to their patient ED population, and how clinicians respond to using the tool.
Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. These patients can be at risk of vomiting and aspiration and often prompts clinicians to pursue definitive airway management to avoid pneumonia and other complications. References: Freund Y et al.
These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED. Did they pick a heap of PEs?
Our guest is trauma surgeon Dr. Dennis Kim ( @traumaicurounds ), associate professor of Clinical Surgery at UCLA and medical director of the Harbor-UCLA Medical Center SICU, as well as host of the Trauma ICU Rounds podcast. pneumatically), then definitively addressed by Orthopedics at their convenience.
The ED clinician should inquire about a relevant history of HIV infection, malignancy, high-dose corticosteroid use, chemotherapy, organ transplant, or use of immunosuppressive drugs for other indications. She reports occasional central chest pain exacerbated by coughing. Int J STD AIDS. 2019;30(2):188-193. Am J Emerg Med. 2013;31(2):401-405.
Also known as Facilitated intubation (FI), the use of intubating with only a sedative was an accepted alternative intubation technique prior to those definitive studies in the late 1990s but quickly was abandoned for RSI in all emergent endotracheal intubations (ETI) (8,9). To date, ketamine has been the agent of choice (12).
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
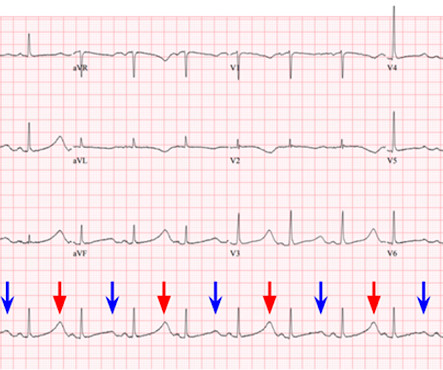
They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2]
A 39-year-old male with history of achalasia with recent endoscopic dilation 24 hours prior presents to the ED for progressively worsening chest pain with radiation to his left shoulder. If there will be a delay in definitive management and there is evidence of intra-thoracic gastric contents, consider chest tube placement.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
2][3] Definitive diagnosis is made by laryngoscopy or bronchoscopy showing normal or mildly erythematous epiglottis and an erythematous, edematous trachea with thick mucopurulent exudates. [3] Labs and x-ray can be nonspecific, and definitive diagnosis is made with direct visualization. ampicillin-sulbactam).
Definitive emotional support is critical to our emotional and psychological well-being. Very rarely are the ED team allowed to stand, in silence, with a purpose. 2018) “Sacred Pause Imitative in the ICU: A survey of ICU physicians and nurses”. This gives rise to feelings of failure alongside the feelings of grief.
A 65 y/o Female was admitted to the ICU for septic shock. They are not premature, by definition. Chou’s Electrocardiography in Clinical Practice (6th ed). Paco Dardon (@PacoDardon), and it’s a privilege to present it as a formal review due to the many pathophysiological, and electrophysiological, phenomenon at play. Surawicz, B.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. A 25-year-old man presents to the ED via EMS after he sustained a gunshot wound to the left flank.
This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. J Med Toxicol. Epub 2019 Jul 3. PMID: 31270748 Maheshwari K, et al. Am J Emerg Med.
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. 2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Paper: Owyang CG, et al. J Crit Care.
On arrival to the ED the patient was intubated with normal vital signs. She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. This patient presented to the ED “after a couple of days of chest discomfort”.
A 53-year-old female with a past medical history significant for hypertension presents to the ED with headache and dizziness. Definitive diagnosis of cerebellar infarction is made with MRI of the brain, as CT imaging (both non-contrast and IV contrast) is often unremarkable and has poor sensitivity for cerebellar stroke.
A biopsy is often ultimately required for a definitive diagnosis. You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? Arch Dis Child Educ Pract Ed. RadioGraphics.
It has been well over a year since the controversial publication of the Agency for Healthcare Research and Quality (AHRQ) report on diagnostic errors in the emergency department (ED). percent of ED visits resulted in preventable death as result of diagnostic error. Further diagnostic testing in the ICU identified salicylate toxicity.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups.
The Importance of Civility in Critical Care Resuscitation A 3-year-old patient with diabetic ketoacidosis arrives at your ED. The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. The junior staff member remains silent throughout the debrief and does not attend their shift the following day.
TTP is a lovely ICU diagnosis. TTP is a lovely ICU diagnosis. Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the usual filters of ED, medical team to the ward. There is a definitely a chance to shine and make the diagnosis.
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). 2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU).
Babie Junior, or Bee for short, was the definition of a cute, delightful baby. You, however, are working an ED shift, and when you see the name “Barbie Junior” on your computer screen, your heart does a flutter. It can be in started in the ED, and many of us are already using it. What were Barbie and Ken to do?
3.6 – 55.6) (-) LR: 0.13 (0.08 – 0.20) ED US (+) LR: 9.5 (2.1 3.6 – 55.6) (-) LR: 0.13 (0.08 – 0.20) ED US (+) LR: 9.5 (2.1 A normal lactate does not rule out the diagnosis Plain X-rays perform poorly in making or ruling out the diagnosis. Louis, Mosby, Inc., 2010, (Ch) 92: p 1216-1227.
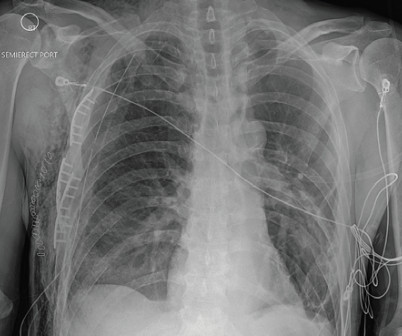
A 58-year-old male with a history of alcohol abuse presented to the emergency department (ED) as a category 2 trauma for a fall with a reported flail chest. Case FIGURE 1: Chest X-ray of multiple rib fractures (arrows). Click to enlarge.) The patient had been drinking with friends when he was witnessed to trip and fall a distance of one step.
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. In the ED, ultrasound showed hemopericardium with tamponade. An ED thoracotomy was done and the pericardium drained and internal compressions continued.
Gibney, MD Originally published: Common Sense March/April 2021 It definitely felt different this new year. I’m pretty sure she was downsized in April because of me and a letter she wrote about her concerns, especially since I would be on the COVID ICU and her coworkers had multiple comorbidities that made them high risk.
This single-centre academic urban institution in the United States (US) undertook a 10-year retrospective observational study of paediatric intubation and bougie use in their emergency department (ED). During a 6-month period, paediatric patients (< 18 years old) who underwent tracheal intubation in their ED were included in the study.
JHS’ chart review project, which identified 163 patients presenting to the ED with gluteal AFT complications in a 30-month period between 2020 and 2023, provides one of the most comprehensive and informative datasets on the breadth of AFT complications as they are currently being performed. units per patient.
The patient vomited once and given the more intense pain decided to come to the ED. 2-hour hsTn: 615 ng/L; bedside ED echo (without contrast) did not show a clear wall motion abnormality (WMA). Tonight’s episode did not improve with simethicone and Tums as it had previously. No history of GIB, dysuria, or GU symptoms. Abstract 556.
Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Of course this must be followed immediately with definitive therapies and potassium source control if possible. Bottom Line: Hyperkalemia is an increasingly common ED diagnosis that must not be missed.
The authors excluded those with devastating injuries (expected to die within one hour of admission), need for thoracotomy prior to receiving blood products, significant burns (>20% total body surface area), inhalation injuries, or receiving over five minutes of cardiopulmonary resuscitation prior to arrival or in the ED.
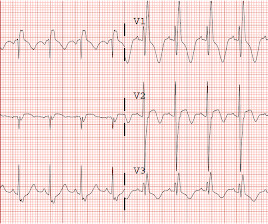
She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? Lead I has a definitively hyperacute T-wave without STE. Clearly, if repeat ECG showed more diffuse, increased ST elevation — a definitive diagnosis of a STEMI would more easily be made. V2 still has STE and hyperacute T-waves.
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. On arrival in the ED, he was hypotensive with a systolic blood pressure in the 70s.
More specific information such as definitive RV diastolic collapse was not indicated or available at this time given the obvious clinical context. We obtained access and monitoring, but she showed no signs of improvement, and we judged that an intervention must be done in the ED without delay. She was discharged home in good condition.
The patient was managed in the ICU and had serial troponins. Figure-1: The first 2 ECGs shown in this case ( See text ). == C OMMENT : As per Dr. Smith — E CG # 1 was the initial tracing on this patient who presented to the ED already intubated for respiratory failure. It is not yet available, but this is your way to get on the list.
As the only respiratory therapist in the ED has been paged and is starting BiPAP for this patient, an overhead call for two incoming trauma alerts from a multivehicle collision sounds. Because the RT responsible for drawing arterial blood gases is busy caring for these patients, ABGs will be delayed. proning patients, ECMO) (12).
A 64-year-old male presents by EMS to the ED with shortness of breath. 1 There are over 50,000 visits related to heart transplant in the United States each year and over half of these patients are admitted to the hospital from the ED. In boarding patients, anti-rejection medications may need to be ordered from the ED.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content