This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
I simply texted back: "Definite posterior OMI." The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration.
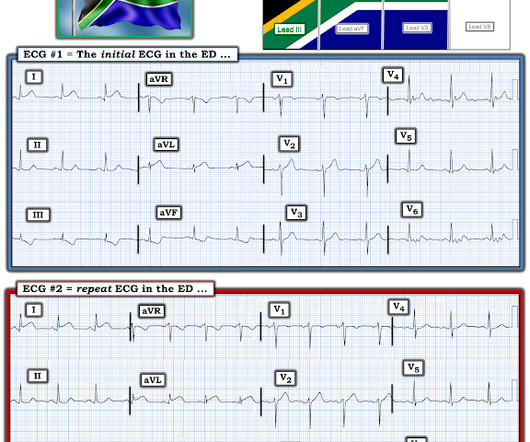
Here is his initial ED ECG: What do you think? Here it is: Obvious Inferior Posterior STEMI (+) OMI. Then the ED doc would be dependent on that first ECG. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Or had not had a prehospital ECG on the ambulance.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." What do you think?
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." The patient was discharged home the next day. No further follow up is available.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. The following ECG was captured upon arrival at the receiving ED.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay.
[link] Case continued She arrived in the ED and here is the first ED ECG. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. I don't know if her pain was getting better or not. From Gue at al.
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. I also told them to get one more 12-lead before they get to the ED. Here is the ECG: What do you think?
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? It is a STEMI equivalent.
The patient was brought to the ED and had this ECG recorded: What do you think? Cardiac arrest #3: ST depression, Is it STEMI? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves.
Self-medicated with 600 mg Ibuprofen and 750 mg Paracetamol (no change) prior to driving to the ED. This is my response: "This is definitely acute or subacute. See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. BP 112/80, SpO2 100%.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. On arrival in the ED, the patient denied any symptoms at all. A 50-something had syncope while driving. He was belted and it was low speed. He had a prehospital ECG.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. RR18 sat 99% HR 90 BP 90/60, afebrile.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting.
In the context of remote rural communities, this can help emergency physicians advocate for their patients, and reduce reperfusion delays by days for STEMI(-)OMI == MY Comment , by K EN G RAUER, MD ( 9/8 /2023 ): == Today’s case is distinguished by its occurrence in a remote rural community ( where the nearest cath lab is a plane ride away ).
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. However, this STE is definitively abnormal in the setting of a normal QRS complex and hyperacute T-wave morphology in V2. The delay between OMI and STEMI sometimes causes unacceptable loss of myocardium or worse.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
This algorithm called it a STEMI. Yet it gave a diagnosis of STEMI. This is, in effect, a transient STEMI 2. See the learning points in that case == Comment by K EN G RAUER, MD ( 3/8/2019 ): == Superb teaching case presented by Dr. Smith regarding this middle-aged man who was transported to the ED after new-onset chest pain.
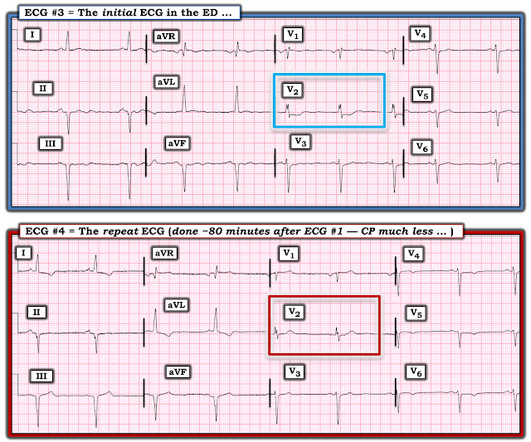
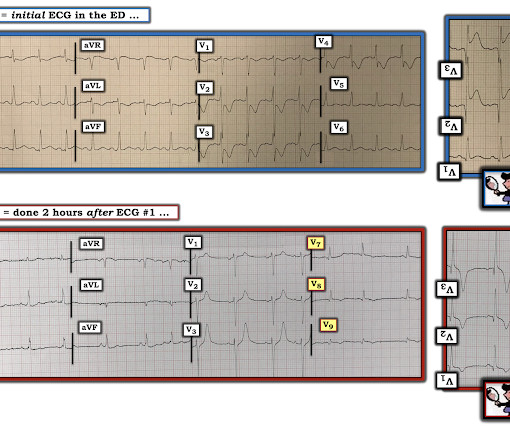
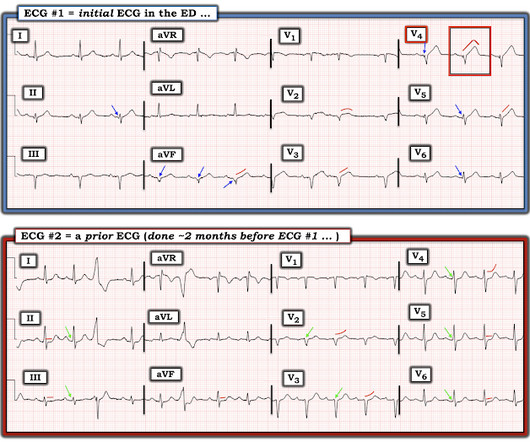
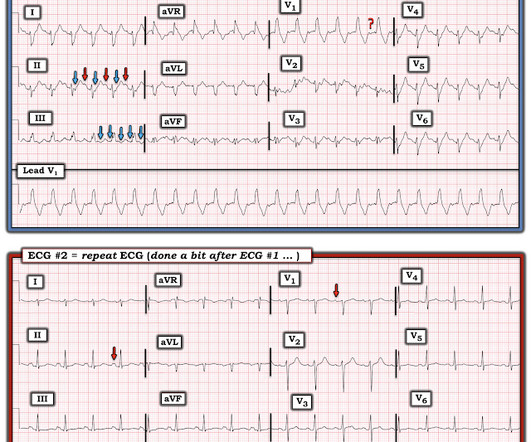
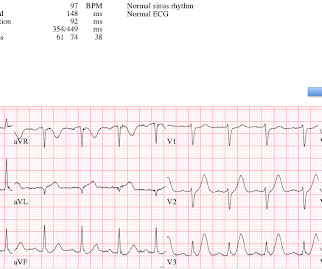
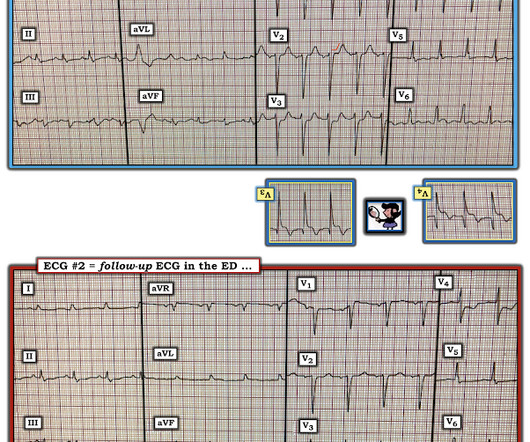
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). 2 Informational: I was provided with a repeat ECG on this patient — which was recorded a bit after ECG #1, still in the ED ( Bottom tracing in Figure-3 ).
He reported typical chest pain since 4H AM and arrived at our ED at 10h with ongoing chest pain. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The first ECG (10h14) showed TWI in inferior leads."
Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. His ED ECG showed his baseline LBBB, with no evidence of MI. So there is a definite inferior and lateral MI. Pendell is the lead author on our Modified Sgarbossa Criteria Validation Study. Limkakeng AT. Theiling BJ.
[link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! They only looked at ED diagnosis, not at any angiogram or even at discharge diagnosis. Fair enough.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Setting – large, academic, suburban ED.
Here is his first ED ECG: What do you see? The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chest pain. Canto et al.
So this is a normal amount of STE in V2 and V3, defined by Universal Definition of MI as up to 2.0 So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Figure-1: The initial ECG done in the ED ( See text ). mm in men over age 40.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Limkakeng AT.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent.
Here is his ED ECG: There is bradycardia with a junctional escape. There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch.
He presented to the ED after 30 minutes, now also feeling weak. Thus, there are some suspicious abnormalities, but no definite signs of ischemia. This abnormality in V3 was apparently not seen by the treating MD, who is a nationally recognized expert in STEMI care (showing how difficult these diagnoses can be).
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. The ED team again pointed out the evidence of inferoposterior OMI, this time by the modified Sgarbossa criteria. The cath lab was activated.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content