This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Chris Root is an emergency medicine and emergency medicine service (EMS) physician at the University of New Mexico, Albuquerque. Chris completed his emergency medicine residency and EMS fellowship at UNM. Before attending medical school, he was a New York City Paramedic. There is drug paraphernalia scattered around the room.
The key is a stepwise, three-pronged approachresuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleedingto keep the patient safe until shes transferred to definitive care. Special thanks to Dr. Kevin Wasko, guest expert on the EM Cases podcast on this topic, who inspired this column.
To celebrate the end of trauma season ( is it ever really over? ), we here at the Ped EM Morsels Bakery have cooked up a morsel to remind you that pediatric trauma can be even more difficult than you think. Definition A series of hemodynamic changes related to autonomic denervation and loss of sympathetic tone. Never fear.
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
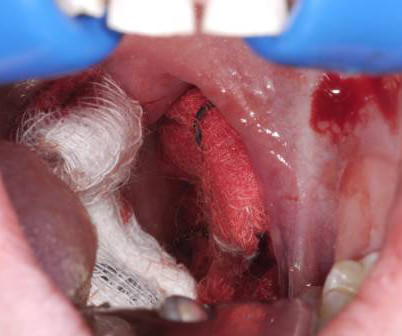
The definitions, typical healing course, timing of bleed, indications for tonsillectomy and the procedure itself have not changed much since our original morsel. Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps.
Yet at the same time, despite a large-scale Holmberg study involving over 6,000 patients suggesting potential harm, epinephrine remained part of the pediatric symptomatic bradycardia protocol. EMS is a unique subspecialty within medicine, and we owe it to our patientsand to ourselvesto dig deeper. The result?
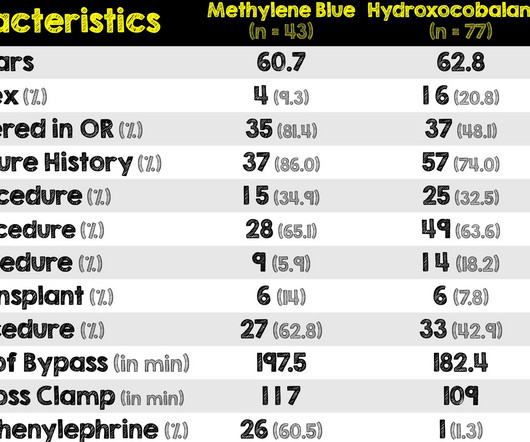
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie (REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia. Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie ( REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia.
EMS arrived and found him in Ventricular Fibrillation (VF). After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% This patient was witnessed by bystanders to collapse. They started CPR. He was defibrillated into VT. sodium bicarbonate.
In cardiac arrest, a delay in IV access subsequently results in a delay in epinephrine administration. Rezaie, MD (Twitter/X: @srrezaie ) The post Don’t Forget About the IO in the Critically Ill Patient appeared first on REBEL EM - Emergency Medicine Blog.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. 5 More recent literature defines “refractory” as VT or VF that is persistent or recurrent despite three shocks from a defibrillator, three rounds of epinephrine, and use of an antiarrhythmic (i.e.,
to 1mg/kg/hr) Information regarding the vasopressors used in the study is as follows: Norepinephrine equivalents = norepinephrine mcg/kg/min + (phenylephrine mcg/kg/min/10) + epinephrine mcg/kg/min + (vasopressin units/min x2.5) REFERENCES: Hiruy A, et al.
At REBEL EM, we’ve done an extensive write up that details some of the different types of DED and the electrophysiology behind it. Within the United States, due to paramedic shortages, this dual-medic setup does not exist in many EMS systems. That write up was for the DOSE-VF pilot trial done in March 2020 and can be found here.
EMS arrived and found her in a wide complex PEA rhythm. She was given 3 mg IV epinephrine and multiple rounds of ACLS over approximately 20 minutes. This is commonly found after epinephrine for cardiac arrest, but could have been pre-existing and a possible contributing factor to cardiac arrest. CPR was started immediately.
Noninferiority trials, covered here on REBEL EM , are helpful when the experimental treatment offers a distinct advantage over the standard treatment. Rezaie, MD (Twitter: @srrezaie ) The post Cetirizine Vs Diphenhydramine For the Treatment of Acute Urticaria in the ED appeared first on REBEL EM - Emergency Medicine Blog. Schaefer P.
Her family called EMS and EMS recorded hypotension and this ECG: What do you think? At about 30 minutes after presentation, the patient had acceptable vital signs with the TVP and low dose epinephrine drip. Figure-1: ECG #1 — recorded by EMS on the scene ( See text ). This is an obvious inferoposterior OMI.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
We’ll keep it short, while you keep that EM brain sharp. 2][3] Definitive diagnosis is made by laryngoscopy or bronchoscopy showing normal or mildly erythematous epiglottis and an erythematous, edematous trachea with thick mucopurulent exudates. [3] A 6-year-old girl presents to the ED with 1 day of fevers up to 104.1°F
Case: EMS arrive to your emergency department with a 68-year-old man post cardiac arrest patient. They had a difficult time getting a definitive airway pre-hospital. It required multiple attempts which caused several prolonged interruptions in CPR. Background: We have covered OHCA many times on the SGEM.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. Epinephrine infusion was begun. There is no definite evidence of acute ischemia. (ie, Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient. Bourke Tillmann and Scott Weingart for their expertise on the EM Cases podcast that inspired this column.
They stated that the patient was coded for 20 minutes, including multiple doses of epinephrine, and they also gave glucose, calcium, and bicarb. As stated above, resuscitation included epinephrine, calcium, and bicarb. He had been given 3 grams Ca gluconate by EMS. After ROSC achieved: Sinus rhythm. QRS much more narrow.
The call involved a sick patient where the student, who was on the verge of going to boards, pulled out the wrong concentration of epinephrine. As they told the story, a couple conversations with the director of EMS, the medical director, and the clinical management, and the student was gone. But not in this case. 3) Anxiety.
Patients exclusively managed in the ICU which decreases applicability for patients in other locations Very small sample size of 96 patients No definition was provided for exclusion criteria of significant cardiopulmonary disease. It’s unclear whether interventions such as cauterization, clip placement, epinephrine injection, etc.,
Likely due to different definitions for hypotension and adverse/major critical events, but the numbers remain higher than we would ever like — Kinda scary when you think about it. Epinephrine should be considered as the vasopressor of choice in patients with decreased myocardial function. Now, what is the resuscitation end goal?
Case: You’re doing a ride along with your local emergency medical service (EMS) crews and responding to an out-of-hospital cardiac arrest (OHCA). The paramedic is trying to get intravenous (IV) access to give epinephrine per the protocol. Epinephrine has long been a cornerstone in the management of OHCA.
Authors: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA); Christian Daniello, MD (Staff Physician, Geisinger Wyoming Valley) // Reviewer: Brit Long, MD (@long_brit) Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. Thats 18 beats per minute.
Earlier in the summer, I wrote a blog discussing the challenges, intricacies, and educational pitfalls of postpartum hemorrhage in EMS. In the standard care of anaphylactoid reactions, we administer Epinephrine, Diphenhydramine, steroids, and bronchodilators. I even know of cases that my colleagues have managed!
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content