This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case: The Chief of Emergency Medicine (EM) at a large urban hospital recently approached the AI Committee at Unity Health, intrigued by the CMAJ article describing the apparent success of CHARTWatch in detecting early signs of patient deterioration. Background: There are many ways to define artificial intelligence.
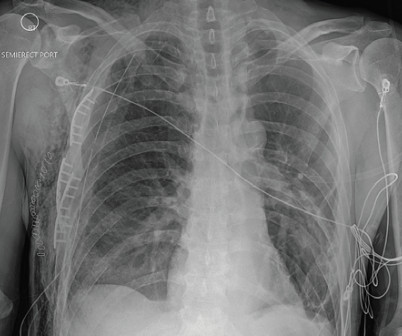
We’ll keep it short, while you keep that EM brain sharp. Disposition: Consider ICU for many patients, especially if any signs of instability or repeatedly requiring blood products. A 25-year-old man presents to the ED via EMS after he sustained a gunshot wound to the left flank. Vital signs include BP 90/48, HR 122, T 98.3
PMID: 35387313 Clinical Question: Do prehospital antibiotics impact 28 day mortality, length of stay in the hospital and ICU length of stay for patients triggering sepsis compared to usual care (No prehospital antibiotics)? appeared first on REBEL EM - Emergency Medicine Blog. to 0.97; p = 0.02 to 2.07; p = 0.91 to 12.33; p = 0.26
Authors: Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA), Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
Case: Johnny is a 22-year-old male patient who presents to the emergency department via EMS with a seizure. He is now stabilized, fosphenytoin is being infused, you are getting ready to ship him to the neuro-ICU and wonder if cooling him down would help. He is known to have poorly controlled epilepsy.
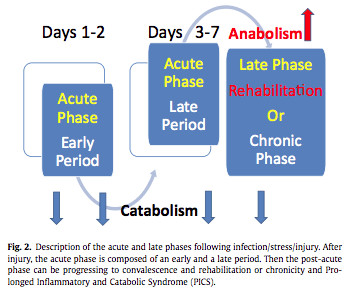
As an EM trainee doing intensive care I will confess that I struggle to work up the enthusiasm to cover a nutrition guideline. As an EM trainee doing intensive care I will confess that I struggle to work up the enthusiasm to cover a nutrition guideline. As with all ICU nutrition EN is preferred over PN. This is the first step.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiac arrest with return of spontaneous circulation. She had an uneventful ICU course and was extubated for ongoing care with the inpatient psychiatric service.
EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest. The post Case Report: EMS Says Flail Chest, But Is It? The patient had been drinking with friends when he was witnessed to trip and fall a distance of one step.
A 65 y/o Female was admitted to the ICU for septic shock. They are not premature, by definition. Paco Dardon (@PacoDardon), and it’s a privilege to present it as a formal review due to the many pathophysiological, and electrophysiological, phenomenon at play. She was critically ill despite aggressive vasopressor therapy.
The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Rezaie, MD (Twitter: @srrezaie ) The post The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults appeared first on REBEL EM - Emergency Medicine Blog. J Med Toxicol. Epub 2019 Jul 3. Intensive Care Med.
A biopsy is often ultimately required for a definitive diagnosis. You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? Why do we worry about the airway? J Thorac Oncol.
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. 2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Paper: Owyang CG, et al. J Crit Care.
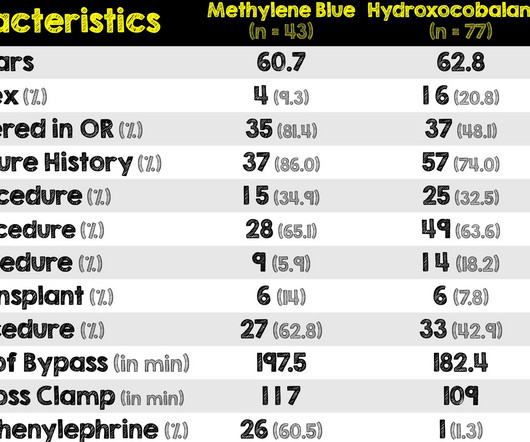
So with yet another confounding variable added (sicker patients at baseline in methylene blue group), the comparison of these two medications is yet again even more difficult There was no difference in ICU and hospital length of stays or hospital mortality between the two groups. REFERENCES: Hiruy A, et al.
Given that a lot of ICU bed days are given over to managing SAH, I felt it might have warranted its own chapter. Though i’ll admit that that question is delving much more into the realm of EM than hard core crit care. The scene fades and the time jumps and the question stem now is in the ICU on day 5.
When you compare it with older definitions like AKIN and RIFLE you can see that not a great deal has changed. While iI hear it is technically possible to get someone admitted to hospital without a CT, it seems that most people I find in the ICU the next day will have had some imaging done (which I really don’t complain about).
I am guilty of over teaching this myself having delivered not one , but 2 talks on the subject, and even a prior tasty morsel of EM on the subject. We definitely see much less of this than we used to. Oh’s manual devotes a whole chapter, number 35 to the subject.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). This could have biased the results in favor of amiodarone as we’ve covered this before on REBEL EM before The IV amiodarone group required less additional HR control agents to control increased heart rate.
These still involve mast cell degranulation) The current guideline accepted definition goes like this serious, life threatening generalised or systemic hypersensitivity reaction that may or may not be immune (ie IgE) mediated While accurate this doesn’t really help me very much in knowing what it looks like. .
We’ll keep it short, while you keep that EM brain sharp. 2][3] Definitive diagnosis is made by laryngoscopy or bronchoscopy showing normal or mildly erythematous epiglottis and an erythematous, edematous trachea with thick mucopurulent exudates. [3] 2][3][9] Glucocorticoid were not shown to alter clinical course or patient outcomes. [2][3]
We’ll keep it short, while you keep that EM brain sharp. Definitive diagnosis of cerebellar infarction is made with MRI of the brain, as CT imaging (both non-contrast and IV contrast) is often unremarkable and has poor sensitivity for cerebellar stroke. Her symptoms have been constant over the last two weeks. 1998; 29(8):1550-1555.
These patients can be at risk of vomiting and aspiration and often prompts clinicians to pursue definitive airway management to avoid pneumonia and other complications. Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. References: Freund Y et al.
3, 4 It is the most common nosocomial infection in patients on mechanical ventilation, and one of the leading causes of nosocomial infection among all patients in the ICU. The low incidence could be a result of the systematic implementation of bundles known to decrease VAP incidence in the ICU. 4, 8 Paper: Dahyot-Fizelier, C.,
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
EMS found her acutely ill, mottled, dry mucous membranes, modestly hypotensive, and lethargic. They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. Thankfully, the patient experienced an uncomplicated ICU stay and subsequently made a full recovery.
In response to this critical issue, the TAME Cardiac Arrest Trial has been launched as a definitive phase III multi-center randomized controlled trial for resuscitated cardiac arrest patients.
Authors: Kamoga Dickson, MD (EM Resident Physician, Makerere University of Health Sciences); Jessica Pelletier, DO (EM Education Fellow, Washington University in St. Consequently, a definitive diagnosis of PJP necessitates the application of molecular, genetic, or direct visualization techniques on IS or BAL fluid to detect PJ.
Also known as Facilitated intubation (FI), the use of intubating with only a sedative was an accepted alternative intubation technique prior to those definitive studies in the late 1990s but quickly was abandoned for RSI in all emergent endotracheal intubations (ETI) (8,9). We don’t want to go backwards!
The TEG group had a shorter ICU length of stay in the first admission. Patients exclusively managed in the ICU which decreases applicability for patients in other locations Very small sample size of 96 patients No definition was provided for exclusion criteria of significant cardiopulmonary disease. Furthermore, 14.3%
EMS Use and Success Rates of Intraosseous Infusion for Pediatric Resuscitations: A Large Regional Health System Experience. undertook a retrospective review of 49 patients aged 0-17 years who had ≥1 EZ-IO insertion attempt by EMS responders in Canada in the context of cardiac arrest or a peri-arrest state if IV access was unobtainable.
They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups. REBOA increased deaths due to bleeding at three hours and 90 days and substantially delayed time to definitive haemorrhage control. c) Or, do both? 2014 Sep;45(9):1287-95.
The definition of massive hemoptysis is variable across publications with expectorated blood volumes ranging from 100 to 1,000 mL per 24 hours, as these volumes are difficult to estimate for any given patient. Bourke Tillmann and Scott Weingart for their expertise on the EM Cases podcast that inspired this column.
He had been given 3 grams Ca gluconate by EMS. Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Of course this must be followed immediately with definitive therapies and potassium source control if possible. Ortho and nephrology were consulted.
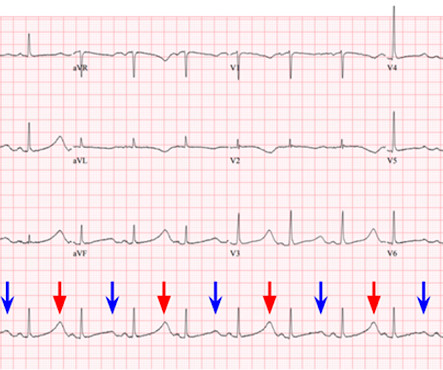
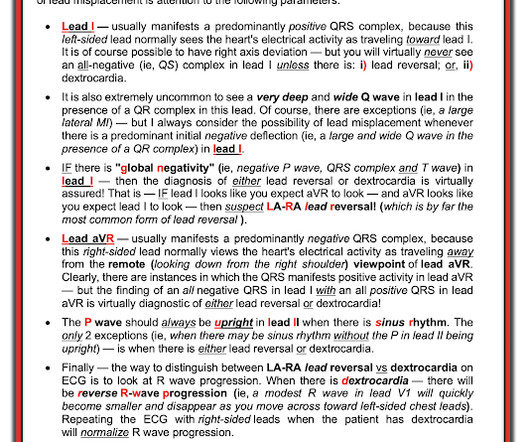
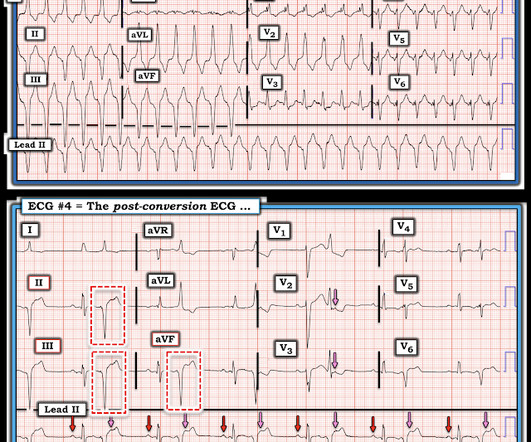
Lead I has a definitively hyperacute T-wave without STE. If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training. V2 still has STE and hyperacute T-waves.
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. EMS arrived and found him awake and alert. The QRS is narrow and T waves are much less peaked.
We’ll keep it short, while you keep that EM brain sharp. A 17-year-old girl, in moderate distress, is brought in by EMS after a motor vehicle collision. EMS reports that she was “pinned” underneath the dashboard, and it took several hours to extricate her. A systematic review on the definition of rhabdomyolysis.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University School of Medicine, St. Louis, MO); Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine, St. We’ll keep it short, while you keep that EM brain sharp. A 64-year-old male presents by EMS to the ED with shortness of breath.
Authors: Rachel Kelly, MD ( EM Resident Physician, Stony Brook University Hospital); Robert Nocito, MD (EM Attending Physician, Stony Brook University Hospital) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University in St. proning patients, ECMO) (12).
4 The 2023 ACORN Trial ( covered here on REBEL EM ) randomized 2,511 patients requiring antipseudomonal coverage to receive either cefepime or piperacillin-tazobactam. independence of the instrument from unmeasured confounders), which cannot be definitively proven in an observational study. In 2021, Buckley et. vs. 52.2%).
That said, complications tied directly to intubation in the field—like aspiration—tend to be more common due to the conditions EMS providers work under compared to the controlled environment of a hospital. "I’d say that EMS providers already do a phenomenal job managing complex airways in challenging conditions. Why is that? "Ketamine
The incidence varies from 2% to 19% depending on the definition of primary. Methods: Adult, non-traumatic OHCA patients in the ESO Data Collaborative 2018-2023 datasets who experienced OHCA prior to EMS arrival, presented with a shockable rhythm, and received amiodarone or lidocaine during resuscitation were evaluated for inclusion.
Well keep it short, while you keep that EM brain sharp. The most appropriate disposition for this patient is admission to an ICU due to increasing oxygen requirements, high mortality rates of IPA, and IDSA recommendation for bronchoscopy with lavage/tissue sampling. COPD, cystic fibrosis), HIV/AIDS, cancer, immunosuppressed (i.e.
Fortunately , you don't need to make a definite diagnosis. She was critically ill and required noninvasive positive pressure ventilation and ICU admission for suspected infectious respiratory illness. But the superior axis with positive QRS in V1 is difficult to reconcile with an accessory pathway.
Authors: Kyle Smiley (EM Resident, BAMC, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Welcome to Critical Kids, an emDOCs series focused on pediatric emergency medicine. Pediatric emergencies are challenging. Well provide summaries of the evidence to support your decisions at the bedside.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content