This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
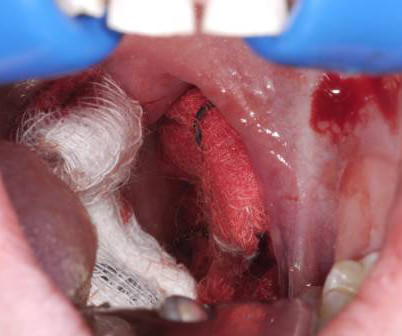
The key is a stepwise, three-pronged approachresuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleedingto keep the patient safe until shes transferred to definitive care. Special thanks to Dr. Kevin Wasko, guest expert on the EM Cases podcast on this topic, who inspired this column.
We’ll keep it short, while you keep that EM brain sharp. F, RR 16, SpO2 97% on room air. A 25-year-old man presents to the ED via EMS after he sustained a gunshot wound to the left flank. His initial vital signs include HR of 116 bpm, BP of 75/50 mm Hg, RR of 25/min, and SpO2 of 98% on room air.
What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operatingroom? How can we best pick up occult cardiogenic shock before it floured shock kicks in? Which patients with acute heart are safe to send home in general?
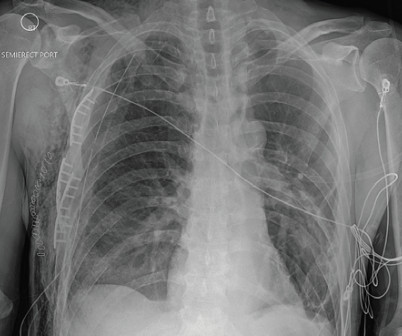
EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest. On hospital day 2, he was taken to the operatingroom for surgical rib fixation. The post Case Report: EMS Says Flail Chest, But Is It? J Surg Res.
Rezaie, MD (Twitter: @srrezaie ) The post The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults appeared first on REBEL EM - Emergency Medicine Blog. Am J Emerg Med. 2016; PMID: 27720568 Guest Post By: Courney Knieriem, MD PGY-1, Emergency Medicine Resident RWJBH Community Medical Center, Toms River, NJ Courtneyknieriem.md@rutgers.edu
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. Rezaie, MD (Twitter: @srrezaie ) The post Impact of Emergency Department Crowding on Lung Protective Ventilation appeared first on REBEL EM - Emergency Medicine Blog.
We’ll keep it short, while you keep that EM brain sharp. Open reduction in the operatingroom may be required if closed reduction is unsuccessful. Overview of OperatingRoom Procedures During Inpatient Stays in U.S. Initial vital signs include T 36.8, HR of 91, BP 138/88, RR 16, SPO2 98% on RA. Hospitals, 2018.
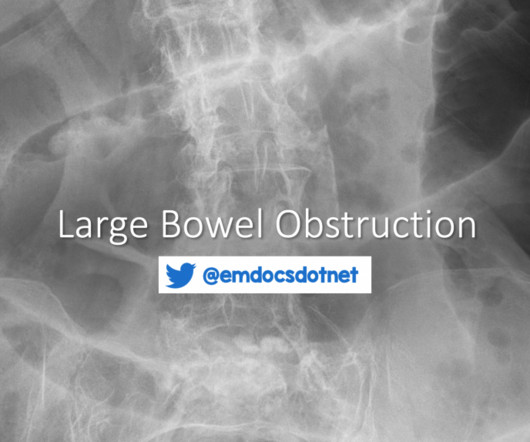
Evaluation Imaging A definitive diagnosis of LBO requires imaging, most often a computed tomography (CT) scan with intravenous (IV) contrast. Symptomatic management for patient comfort with antiemetics and analgesics, while definitive management is undertaken, should not be overlooked. This also serves as a tool for surgical planning.
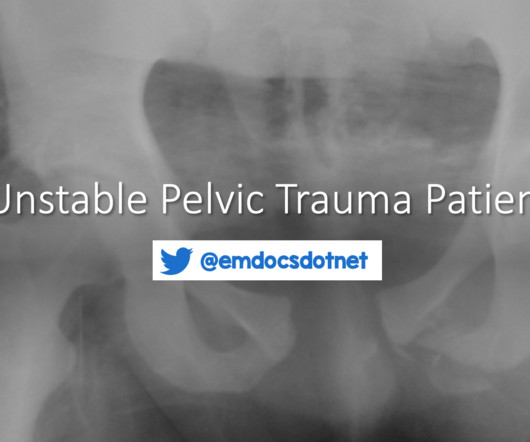
C, respiratory rate 20 breaths per minute, and oxygen saturation 95% on room air. What is the EM physician’s role in the stabilization of unstable pelvic injuries? If a pelvic binder was placed by EMS, inquire whether this was placed empirically or if mechanical pelvic instability was already elicited.
Temporomandibular (TMJ) Joint Dislocation Definition: Displacement of the mandibular condyle from the temporomandibular fossa. Rezaie, MD (Twitter/X: @srrezaie ) The post REBEL Core Cast 133.0 – TMJ Dislocation appeared first on REBEL EM - Emergency Medicine Blog. Philadelphia: Elsevier Saunders, 2014.
Earlier in the summer, I wrote a blog discussing the challenges, intricacies, and educational pitfalls of postpartum hemorrhage in EMS. Definitive care for an intrapartum cardiac arrest is a maternal perimortem cesarian section, which may be performed by any emergency physician. I even know of cases that my colleagues have managed!
An EM Residents Guide to Basic Airway Management Authors: Justin Rice, MD Sagar Desai, MD Eunice Monge, MD William Chiang, MD Preface: Airway management is one of the most critical skills in emergency medicine, yet it can be one of the most challenging to master. But note the excellent opportunity for IV access in the EJ. Auscultation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content