This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
One definition of AI is a computer system capable of performing tasks that typically require human intelligence, such as pattern recognition, decision-making, and language processing. By alerting clinicians to potential problems before they become critical, AI-driven systems aim to reduce unplanned ICU transfers and improve survival rates.
Definition A rapidly progressive, life-threatening infection of the deep soft tissues. Surgical Consultation Early surgical exploration is often the definitive diagnostic step. Not definitive but can guide suspicion. Supportive Care Intensive monitoring, often in an ICU setting.
PMID: 35387313 Clinical Question: Do prehospital antibiotics impact 28 day mortality, length of stay in the hospital and ICU length of stay for patients triggering sepsis compared to usual care (No prehospital antibiotics)? to 0.97; p = 0.02 to 2.07; p = 0.91 to 12.33; p = 0.26 to 0.97; p = 0.02 to 2.07; p = 0.91 to 12.33; p = 0.26
We look at the rib fracture patient requiring ICU admission, including a discussion of surgical repair, with Dr. Ron Barbosa (@rbarbosa91), Portland trauma surgeon and SICU director at Legacy Emmanual Medical Center. ICU admission in rib fracture patients is still most often a matter of clinician judgment and bed availability.*
Our guest is trauma surgeon Dr. Dennis Kim ( @traumaicurounds ), associate professor of Clinical Surgery at UCLA and medical director of the Harbor-UCLA Medical Center SICU, as well as host of the Trauma ICU Rounds podcast. pneumatically), then definitively addressed by Orthopedics at their convenience.
A look at oncology-related emergencies in the ICU, with Leon Chen (@CCMNP), NYC nurse practitioner specializing in oncology critical care. Acyclovir for viral prophylaxis and posaconazole for fungal (galactomannan and beta-d glucan are helpful)* The blast count is suggestive of leukemia, but definite diagnosis will require bone marrow biopsy.*
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs. WOMAN are so negative WOMAN-2 Trial Collaborators.
He is now stabilized, fosphenytoin is being infused, you are getting ready to ship him to the neuro-ICU and wonder if cooling him down would help. His oxygen saturation begins to drop and you decide to intubate and mechanically ventilate. Background: We have covered hypothermia a number of times on the SGEM.
2 Despite advances in imaging and surgical methods, overall mortality approaches 20%, which doubles to 40% with delays to definitive management exceeding than 24 hours. If there will be a delay in definitive management and there is evidence of intra-thoracic gastric contents, consider chest tube placement. May not be an option.
With my deepest apologies to all the great ICU dieticians I have worked with, I just struggle to get excited over this stuff. I would highly recommend attending an excellent lecture given by your ICU dietician which is just possibly where this entire summary came from. As with all ICU nutrition EN is preferred over PN.
A 65 y/o Female was admitted to the ICU for septic shock. They are not premature, by definition. Paco Dardon (@PacoDardon), and it’s a privilege to present it as a formal review due to the many pathophysiological, and electrophysiological, phenomenon at play. She was critically ill despite aggressive vasopressor therapy.
Disposition: Consider ICU for many patients, especially if any signs of instability or repeatedly requiring blood products. The time taken to measure serum hemoglobin and hematocrit (B) and await a result would delay definitive surgical control of likely ongoing hemorrhage given this patient’s incomplete response to fluid resuscitation.
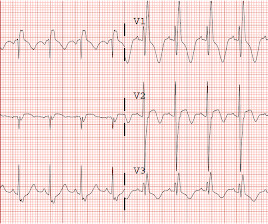
She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. She had an uneventful ICU course and was extubated for ongoing care with the inpatient psychiatric service.
The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Potential to Impact Current Practice: Initiatives should be made at the institution level to develop in-service education sessions, policies and procedures for the safe administration of PDPs in the acute hypotensive period. J Med Toxicol.
However in ICM there is a need to have a broad understanding of what some of the haematological acronyms might mean given that a fair number of these patients end up in the ICU. Most of this post will be navigating the basics of the diseases rather than super specific ICU management. Sepsis is probably number 1 on the list.
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. 2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Paper: Owyang CG, et al. J Crit Care.
The major barrier to implementation in the ICU setting is the almost complete absence of ICU patients from these trial cohorts. And as we all know if there is a complication possible it’s almost definitely going to happen with greater frequency in the ICU cohort. LDH>1000 Sugar <2.2
A biopsy is often ultimately required for a definitive diagnosis. You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? Why do we worry about the airway?
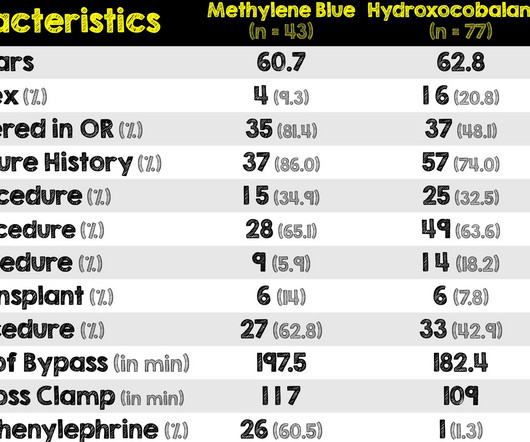
So with yet another confounding variable added (sicker patients at baseline in methylene blue group), the comparison of these two medications is yet again even more difficult There was no difference in ICU and hospital length of stays or hospital mortality between the two groups. REFERENCES: Hiruy A, et al.
This can be found in ~20% of cirrhotics and the key clinical finding is hypoxia that gets better when lying flat, otherwise known as platypnea-orthodeoxia which is probably more common in ASDs but hepatopulmonary syndrome is definitely on the list. The pathogenesis is unclear but nitric oxide plays a role.
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. Is this: 1. The QRS duration measured in lead II (shown below) is about 6.5
ICU level pre eclampsia is. ICU level pre eclampsia is rare. And given that the definitive treatment is removing the baby from the mother, it turns out that this will typically have been done before we even get involved. Firstly some definitions. Read More » Welcome back to the tasty morsels of critical care podcast.
SBS is not a common thing to find in the ICU and the most likely context here is going to be receiving someone from the operating theatre who has had. There are some poor souls who as a result of SBS are dependant on long term TPN who may also appear in ICU from time to time and a working knowledge would be useful.
TTP is a lovely ICU diagnosis. TTP is a lovely ICU diagnosis. There is a definitely a chance to shine and make the diagnosis. Welcome back to the tasty morsels of critical care podcast. Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the.
Given that a lot of ICU bed days are given over to managing SAH, I felt it might have warranted its own chapter. Given that 85% of SAH is aneurysmal, and they need definitive treatment likely not available in your hospital then getting that angio done is certainly a priority. Welcome back to the tasty morsels of critical care podcast.
The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. The lack of consistent definitions in the literature makes it difficult to report its true prevalence and hampers efforts to combat it. How do you manage this situation?
We talk a lot about cerebral protective measures in the ICU and hopefully this will give you a little of the basic physiological background. The brain apparently receives 15% of the cardiac output, though I imagine by the end of a typical ICU on call shift, that proportion will have dropped quite significantly.
When you compare it with older definitions like AKIN and RIFLE you can see that not a great deal has changed. While iI hear it is technically possible to get someone admitted to hospital without a CT, it seems that most people I find in the ICU the next day will have had some imaging done (which I really don’t complain about).
Plasmapheresis (or PLEX) is one of the machines we tend not to have responsibility for in the ICU. Plasmapheresis (or PLEX) is one of the machines we tend not to have responsibility for in the ICU. Unlike CRRT we tend to defer to another specialty to do this. Read More » Welcome back to the tasty morsels of critical care podcast.
We definitely see much less of this than we used to. I suspect that’s largely due to better access and provision of primary care but there remains a cohort of fairly brittle folk out there who will occasional crop up in resus or the ICU. Oh’s manual devotes a whole chapter, number 35 to the subject.
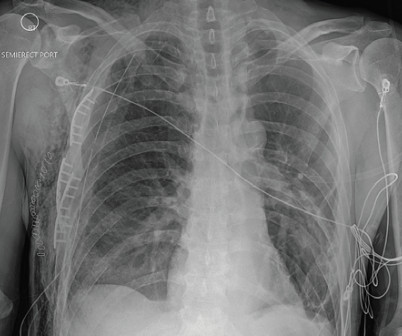
The chest X-ray showed multiple displaced right rib fractures and chest wall subcutaneous emphysema without definitive evidence of a pneumothorax, as well as right lower lobe atelectasis versus contusion (Figure 1). Trauma imaging was performed including bedside X-rays of the chest and pelvis.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Unfortunately, without knowing what dose and at what time first line medications were given before second line agents were administered, precludes any definitive conclusions from being made regarding this trial.
Gibney, MD Originally published: Common Sense March/April 2021 It definitely felt different this new year. I’m pretty sure she was downsized in April because of me and a letter she wrote about her concerns, especially since I would be on the COVID ICU and her coworkers had multiple comorbidities that made them high risk.
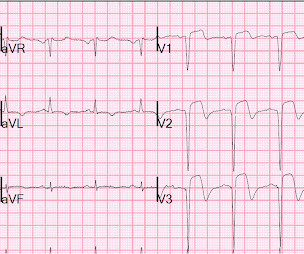
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. Normal RBBB has no ST elevation in any lead, though sometimes there is an exception when there is abscnce of R'-wave, as in V2 here.
These still involve mast cell degranulation) The current guideline accepted definition goes like this serious, life threatening generalised or systemic hypersensitivity reaction that may or may not be immune (ie IgE) mediated While accurate this doesn’t really help me very much in knowing what it looks like.
Definition: total loss of R-wave means there is a QS-wave (a single deep deflection). The patient continued to have ischemia after PCI, and in fact had an episode of polymorphic VT shortly after while in the ICU. Persistence of ST elevation helps to determine state of the myocardium after reperfusion. This was recorded 2.5
The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. Repeat ECG: The cath lab at our nearest referral center was contacted while the patient was in CT and again following the results and repeat labs.
12–13 These are challenging studies to draw definitive conclusions from, however they suggest that some of these post-TTM1 patients who were cooled to 36 degrees Celsius did worse, supporting the notion that there exists a subset of patients who benefit from cooling to 33 degrees Celsius. Crit Care Med. 2020;48(3):362-9. Resuscitation.
The patient was managed in the ICU and had serial troponins. Finally — there has been further evolution of the subtle ST-T wave abnormalities in leads V2, V5 and V6 — which now all show definite ST-T wave flattening in ECG #2. It is not yet available, but this is your way to get on the list. He had no more ECGs recorded. First was 2.9
More specific information such as definitive RV diastolic collapse was not indicated or available at this time given the obvious clinical context. A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content