This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
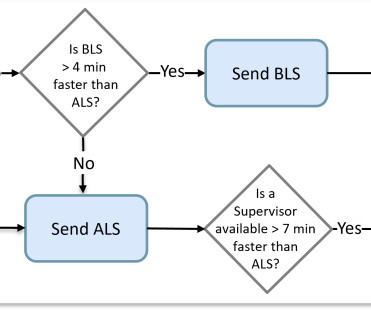
The very low risk calls can typically be satisfied with basic lifesupport (BLS) capabilities. In fact, sending advanced lifesupport (ALS) providers that are in short supply to one of these calls can leave citizens exposed when a critical request is received after that resource is committed.
On November 14, 2024, ILCOR released their latest recommendations for adult and pediatric basic and advanced lifesupport. Many showed positive trends, yet because each specific area had fewer than three supporting articles, ILCOR declined to make any definitive statements about their effectiveness. The result?
Treatment of cardiac arrest and life-threatening toxicity due to poisoning often requires specialized treatments that most clinicians do not use frequently such as antidotes and venoarterial extracorporeal membrane oxygenation, in addition to effective basic and advanced lifesupport. COR 2a, LOE C-LD. COR 2a, LOE C-LD.
When I saw the ECG of this patient I saw that there was definitely something "off". Cardiac arrest was called and advanced lifesupport was undertaken for this patient. Are these ECG changes related to the CNS infection perhaps? What disease processes would you put on your list of differential diagnoses?
More recent literature and guidelines support the use of lidocaine as an alternative agent, and currently both are included in standard advanced cardiovascular lifesupport. Medications: think about using esmolol Amiodarone has been traditionally used in the management of VT or VF as an adjunct to defibrillation.
The search contained terms for (1) prehospital cardiac arrest or prehospital advanced lifesupport, and (2) injuries and trauma. Inclusion/Exclusion criteria and definitions were very specific. The OPALS Major Trauma Study: impact of advanced life-support on survival and morbidity. 2008 Apr 22;178(9):1141-52.
Once we've gotten to the stage where the patient has developed significant pulmonary edema and has suffered tissue damage from the conversion of CL2 to HCL and HOCL, the definitive treatment is pulmonary lavage in hospital and long-term management. Advanced Hazmat LifeSupport Provider Manual (4th ed.). (F. Bronstein, A.
In 2010, the American Heart Association (AHA) revised the Advanced Cardiac LifeSupport (ACLS) guidelines to include the recommendation of using capnography to monitor end-tidal carbon dioxide (ETCO2) during cardiopulmonary resuscitation (CPR), 1 and has continued this recommendation to date. 2011;123:e236].Circulation. Circulation.
Unfortunately, without knowing what dose and at what time first line medications were given before second line agents were administered, precludes any definitive conclusions from being made regarding this trial. Clinical Bottom Line: Numerically, amiodarone may be a better medication for rate and rhythm control. Am J Emerg Med. 2022 Sep 7.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal lifesupport). A followup ECG was recorded 2 days later: No definite evidence of infarction. An elderly woman had sudden ventricular fibrillation. pulmonary embolism, sepsis, etc.), myocarditis).
12–13 These are challenging studies to draw definitive conclusions from, however they suggest that some of these post-TTM1 patients who were cooled to 36 degrees Celsius did worse, supporting the notion that there exists a subset of patients who benefit from cooling to 33 degrees Celsius. N Engl J Med. 2013;369(23):2197-206.
Tactical EMS providers must be able to recognize the signs of non-compressible hemorrhage and initiate rapid evacuation to a medical facility where definitive care can be provided. While these personnel may not be directly integrated into the SWAT team, they are on standby to provide rapid medical support in the event of an injury.
It’s difficult to definitively say which of the two is statistically better, however there is a trend pointing toward DED. The fragility index of these findings found to be 1 for VC and 9 for DED Obtaining a second defibrillator in the emergency department or intensive care unit can be very easy to do.
In your role as an EMT, you would concentrate on immobilizing the area and offering quick transportation for definitive care. They demand urgent medical care because they produce excruciating pain and an obvious deformity.
Before BLS, or Basic LifeSupport, was able to administer Narcan, agencies would have to wait for a MICP unit to arrive on scene to administer the lifesaving medication. Recent studies , however, show that back-boarding patients leads to an increase in agitation, discomfort, and has the possibility of airway compromise.
In the most basic, simplest definition, what is an MCI? In addition to completing a state approved course, you must also have a current CPR-BLS certificate (basic lifesupport). As you have lights and sirens, they will always get out of your way. Correct Incorrect Question 3 of 10 3.
Once SAH has been identified, management should be focused on preventing hematoma expansion, preventing re-bleed, limiting delayed ischemia, reducing intracranial pressure, and preparing for definitive management. 2 These patients also warrant early consultation by neurology and neurosurgery for definitive intervention and management.
Current Advanced Trauma LifeSupport guidelines require all trauma patients to receive intravenous access, and as such it is essential for EMS clinicians to be conversant with situations which may require fluid resuscitation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content