This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
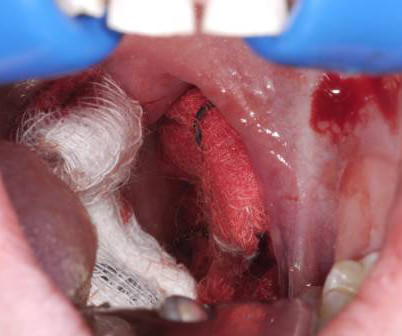
The key is a stepwise, three-pronged approachresuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleedingto keep the patient safe until shes transferred to definitive care. Secondary post-tonsillectomy hemorrhages often require surgical intervention.
What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operatingroom? How can we best pick up occult cardiogenic shock before it floured shock kicks in? Which patients with acute heart are safe to send home in general?
Takeaway lessons * Trauma patients who are hypotensive or otherwise unstable should be assumed to be bleeding, bleeding, bleeding until proven otherwise, and should have a very low threshold to proceed directly to the operatingroom for exploration.* pneumatically), then definitively addressed by Orthopedics at their convenience.
In this patient with a penetrating posterior flank injury, trace-free fluid in the pelvis on eFAST, and ongoing signs of hemorrhagic shock despite fluid and blood product administration, transferring to the operatingroom for exploration is indicated, especially with high probability of zone III injury-related retroperitoneal bleeding.
Might his examination be enough to convince the urologists to take him straight to the operatingroom without a preceding diagnostic ultrasound? Ultrasound imaging of the scrotum is the gold standard for diagnosis of testicular torsion, however can lead to delays in definitive care.
The standard care in North America for post-traumatic EDH involves decompressive craniotomy or trepanation via a burr hole, typically performed in an operatingroom by neurosurgery teams. 2) The EZ-IO® device may be a temporizing and lifesaving intervention until definitive neurosurgical care can be obtained.
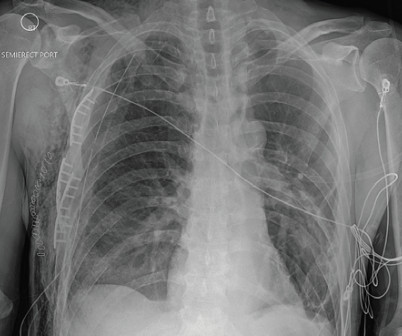
The chest X-ray showed multiple displaced right rib fractures and chest wall subcutaneous emphysema without definitive evidence of a pneumothorax, as well as right lower lobe atelectasis versus contusion (Figure 1). On hospital day 2, he was taken to the operatingroom for surgical rib fixation.
Potential to Impact Current Practice: Initiatives should be made at the institution level to develop in-service education sessions, policies and procedures for the safe administration of PDPs in the acute hypotensive period.
Tracheo-innominate fistula (TIF) is an unusual and frequently lethal complication of such definitive airway placement. 15 Definitive Treatment Definitive treatment of TIF has traditionally involved median sternotomy and ligation of the innominate artery. He has had a tracheostomy for approximately 15 months since his injury.
A search for Brazilian Butt Lift (BBL) on any social media platform will yield thousands of before-and-after images, faja sales, operatingroom videos, recovery tips, and patients praising their plastic surgeon. 9 PFE is only definitively diagnosed on autopsy and a high clinical suspicion must be maintained in high-risk patients.
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. Traditionally patients were managed on the ventilator with lung volumes of 10 – 15 ml/kg.
Open reduction in the operatingroom may be required if closed reduction is unsuccessful. Overview of OperatingRoom Procedures During Inpatient Stays in U.S. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. Hospitals, 2018. 2021 Aug 31. 2024 Sep;34(5):633-640.
Figure 1: The Young-Burgess classification of pelvic ring fractures (source: [link] 3 It is paramount to differentiate the definitions of “hemodynamically unstable” and “mechanically unstable” pelvic fractures. For a broader overview of pelvic trauma, please review Dr. Lupez’s 2017 article here: [link].
of hospitals reported that they had to transfer patients, leading to delays in definitive care. Time is testicle , reminding us that the sooner we get a definitive diagnosis and treatment, the more likely we are to save future generations. This dropped to 79.3%
Evaluation Imaging A definitive diagnosis of LBO requires imaging, most often a computed tomography (CT) scan with intravenous (IV) contrast. Symptomatic management for patient comfort with antiemetics and analgesics, while definitive management is undertaken, should not be overlooked. This also serves as a tool for surgical planning.
6,13,17 Challenges in Diagnosis: The diagnosis of Fournier’s gangrene is clinical: There are no laboratory or imaging studies that can be used to definitively rule out disease. 20,21 Imaging may be helpful in diagnosis or surgical planning but cannot rule out NSTI and may delay definitive surgical management.
CT is more definitive but can take more time. Other exceptions are patient refusal, patient death or immediate transfer to the operatingroom. Bedside US can confirm the presence of AAA, but visualization of the actual rupture may be more difficult because most AAAs rupture into the retroperitoneal space.
Obstetrics and Gynecology was consulted for definitive management. The patient was taken to the operatingroom for dilation and curettage and was discharged the following day.
Definitive care for an intrapartum cardiac arrest is a maternal perimortem cesarian section, which may be performed by any emergency physician. However, despite that, my mind kept going back to the female patient who suffered an intrapartum cardiac arrest.
For an unstable patient in the ED, you will definitely not be able to do this entire evaluation, but any part will be helpful – even if its just having them range their neck and thrust their jaw while getting pre-oxygenated, or looking in the mouth to make sure the jaw isnt wired shut! Auscultation. Observation of chest rise.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content